CIHR Funding Pressures resulting from High Impact Health Infrastructure Investments
July 2007Table of Contents
- Executive Summary
- Acknowledgements
- Project Description and Magnitude of High Impact Investments
- Background
- Objectives
- Conceptual Framework: Definitions
- Project Scope and Methods
- Investments in High Impact Health Infrastructure Projects
- Time Required to Complete High Impact Health Projects
Types of Expenditure for High Impact Projects
- Analysis of CFI project reports for high impact health projects
- State of Development - Ability to Support Research
- Utilization and Funding Issues
- Degree of Utilization
Useful Years Remaining
Operating and Maintenance Funding
Impact on Major Sources of Funding
Researchers and Technicians
Discussion
- CIHR Experience with High Impact Infrastructure Awards
- British Columbia Cancer Research Centre
- Institutions with at least $15 million in CFI high impact awards.
- Major Science Investments
- Summary of Interviews
- Research Directions
- User Fees and Operating Costs
- Planning and Budgeting for Infrastructure
- Research Planning
Financial Planning
- Research Directions
- Projections of Grant Funding Pressures
- Approach 1: Number of Recruits
- Discussion
- Approach 2: Value of funded research Required to Justify Infrastructure InvestmentsComparison of Approaches
- Approach 1: Number of Recruits
- Conclusions
- Appendix
- References
Executive Summary
This project has been undertaken to estimate the impact of large scale infrastructure investments on the present and future demand for health research operating grant funding.
High impact health infrastructure investments are defined for this project as projects with awards from the Canada Foundation for Innovation (CFI) of at least $1 million, which would be equivalent to a total project value of $2.5 million or more with matching funds from institutions and provincial governments. There have been 239 high impact health infrastructure project awards announced since 1999 with a total investment value of $2.9 billion. This excludes the roll-out of awards related to CFI's Hospital Research Fund estimated to have a value of $500 million.
High impact health infrastructure projects represent a major contribution to Canada's research capacity. New state-of-the-art facilities and scientific equipment are increasing the potential of Canada's research community. This new infrastructure has played a large role in attracting world-class researchers from other countries. An understanding of research grant funding pressures resulting from high impact infrastructure projects constitutes a major challenge for CIHR and for governments that understandably wish to achieve the most productive use of infrastructure to which public funds have been committed. This report constitutes an attempt to assemble factual data and insight from experts in the research community that will help to understand present and future funding pressures from new high impact infrastructure.
High impact projects often take a number of years to complete. The major impact of these projects on health research funding requirements has just become evident in the last two to three years and will continue to grow throughout the remainder of the present decade.
High impact health infrastructure projects include new construction, state-of-the-art equipment, research platforms and renovations to accommodate labs or equipment. Equipment and renovations account for approximately 70% of high impact investments. Equipment and renovations have a relatively short useful life span for research (7 years on average, according to senior stakeholders) and timely access to research funding is important if their research potential is to be realized.
CFI provided aggregate data for this study based on 161 CFI project progress reports from high impact health projects that were in their five-year reporting cycle during 2006 or 2005. These projects were funded between 2000 and 2005. Most of the projects are presently in a state of partial development. Most but not all projects reported that infrastructure in place was being fully utilized at its current state of development, which affirms the scientific relevance of these projects. Over 4,000 researchers have furthered their research through association with the projects. Over 1,400 researchers have been recruited to the institution hosting the infrastructure projects, 40% of them recruited from countries other than Canada.
Researchers in high impact health projects report that the greatest impact of the projects on new funding occurs with the traditional sources, particularly federal and provincial granting agencies and the institutions that host the projects. Fully and partially developed projects report different degrees of impact on funding from Canadian industry, which could signal a greater willingness of industry to invest in projects that are fully operational and/or have an established track record. This issue deserves further research in view of public policy to encourage greater participation by the private sector in funding research.
High impact health infrastructure projects are concentrated among nineteen academic and healthcare research institutions. These institutions have increased their shares of CIHR grant funding dramatically since 1999-2000. The success these institutions have achieved with both CFI and CIHR could be interpreted as an indication that they have positioned themselves to play leading roles in future research through strong recruitment and planning. Their funding needs will increase as their high impact infrastructure projects are completely developed.
CIHR, CFI and other partners are funding a small number of major initiatives that are generating or are expected to generate major research activities in Canada. These high impact projects include the Canadian Light Source (presently used by 400 to 500 scientists across Canada), the CFI & CIHR Clinical Research Initiative (announced January 2007), The Structural Genomics Consortium and The Research Data Centres National Network (13 centres used by 1,400 researchers in 2006). Most of these initiatives are multidisciplinary and support research activities throughout Canada.
Interviews with senior stakeholders at health research institutions found agreement that new infrastructure has influenced the development of collaborative research using highly sophisticated equipment and complex techniques. These developments have led to new research methods and approaches. Average grant size is increasing as a result and is expected to continue to increase as new high impact infrastructure becomes a dominant force in health research.
Research grants help to cover operating costs of new infrastructure as well as direct research costs. Without research grants, institutions must either subsidize research with funding from internal sources or maintain new infrastructure that is used below its potential. The limited time in which most new technology remains state-of-the art for research increases the urgency of resolving this problem. Concerns have been expressed about potential under-utilization of new infrastructure due to an imbalance between infrastructure and research grant funding.
Research planning is evolving towards a model that seems to link two different cultures: the traditional investigator led approach to research and the planned collaborative approach that some observers believe is becoming the new paradigm in major research initiatives. This development is affecting recruitment, infrastructure and research planning.
Financial planning has been affected by the availability of infrastructure funding. In addition to CFI supported projects, provinces and institutions are building new life sciences centres or research hospitals. Internal support from foundations and contributions from wealthy donors are increasing in importance as sources of funding for these new facilities. Financial planning is largely focused on infrastructure at present. The amount or value of funded research required to justify infrastructure investments is not normally considered when planning for increased research capacity at the institutional level.
Two approaches were used to forecast present and future funding pressures from high impact health infrastructure projects:
- In the first approach, simulations of funding pressures from researchers recruited to high impact infrastructure indicate that grant funding pressures for CIHR will be approximately $200 to $240 million in fiscal 2007-2008.
- The second approach uses a financial planning model, which assumes that new infrastructure should result in growth of funded research at least equal to the investment and operating costs of the infrastructure. Those simulations indicate that for every $1 billion invested in new high impact infrastructure, research grant pressures can be expected to increase by $270 million. This second approach forecasts funding pressures for CIHR of $243 million in fiscal 2007-2008.
Both approaches forecast funding pressures from high impact health infrastructure in the area of $400 million for CIHR by the end of the decade. A steady state requirement of this magnitude can be foreseen in future years, assuming that future high impact infrastructure investments will be directed to maintaining the considerable gains in research capacity that are being developed at present.
![]()
Acknowledgements
CIHR wishes to acknowledge the following organizations and individuals who made valuable contributions to this report.
Canada Foundation for Innovation
Dr. Eliot Phillipson, President and CEO
Meg Barker, Director, Planning and Outcome Assessment
Peter Potsepp, Project Officer
University of British Columbia
Dr. Don Brooks, Associate Vice-President Research
Brent J. Sauder, Director, Office of Research Services
Twelve senior executives of academic research institutions provided insight and advice through telephone interviews. Six research project leaders provided information used in the analysis.
Interview Participants
Dr. Carl Breckenridge
Vice-President, Research
Dalhousie University
Dr. Don Brooks
Associate Vice-President (Research)
University of British Columbia
Dr. Pierre Chartrand
Vice-President, Research
Canadian Institutes of Health Research
Dr. Tom Feasby
Vice-President, Academic Affairs
Capital Health Authority, Edmonton
Dr. Ken Hastings
Montreal Neurological Institute
McGill University
Dr. Peter Liu
Scientific Director, Institute of Circulatory and Respiratory Health, CIHR
Professor of Medicine and Physiology, Toronto General Hospital Research Institute
Dr. Alex MacKenzie
Vice President, Research
Children's Hospital of Eastern Ontario
Dr. Chris Paige
Vice-President, Research
University Health Network, Toronto
Dr. Mark Poznansky
President and Scientific Director
Robarts Research Institute
Dr. William Tomlinson
Executive Director, Canadian Light Source
University of Saskatchewan
Dr. Jacques Turgeon
Vice-Rector (Research)
Université de Montréal
Dr. Bruce Waygood
University Coordinator of Health Research
University of Saskatchewan
Project leaders and others who provided information and advice
Dr. Pavel Hamet
Professor, Faculty of Medicine, Université de Montréal
Associate Professor, Department of Medicine, McGill University
Director of Research and Endocrinologist, Centre hospitalier de l'Université de Montréal
Paul O'Byrne
EJ Moran Campbell Professor,
Chair, Department of Medicine,
McMaster University
Dr. Gary Lopaschuk
Scientific Director, Mazankowski Alberta Heart Institute
Professor, Depts. Pediatrics and Pharmacology
University of Alberta
Dr. Bruce McManus
Professor, Department of Pathology and Laboratory Medicine
Director, iCAPTURE Centre, Providence Health Care
University of British Columbia
Janet Northan
Director, Cancer Research, Innovation and Planning Regional Cancer Care
Thunder Bay Regional Health Sciences Centre
Dr. Arthur S. Slutsky
Vice President (Research), St. Michael's Hospital
Professor of Medicine, Surgery and Biomedical Engineering
Director, Interdepartmental Division of Critical Care, University of Toronto
Officials from Finance Canada and Industry Canada participated in presentations of preliminary findings in January and offered helpful comments and advice.
CIHR staff who were instrumental in developing this report include:
Terry Campbell, Executive Director, Strategic Policy and Government Relations
Elissa Hines Reimer, Senior Policy Advisor
Andrew McColgan, Senior Policy Advisor
This report was prepared under contract by: Vern Hicks, Health Economics Consultant
![]()
Project Description and Magnitude of High Impact Investments
Background
The federal government has made large investments in research capacity since 1997. These investments included support for infrastructure (Canada Foundation for Innovation (CFI) starting in 1997) and for human capital (Canada Research Chairs (CRC) starting in 2000). Direct research funding support increased through the establishment of CIHR (2000) and the Indirect Cost program (2003). Federal research funding in 2004-2005 was valued at $1.286 billion, of which CIHR expenditures accounted for $757 million.i
Coincident with these changes, university enrollment increased, leading to increases in faculty positions. All these trends have occurred within an evolving cultural awareness of the value of knowledge as a means to further economic and social progress. The demand for research has increased as a result and is continuing to increase.i
High impact infrastructure projects have contributed significantly to the ability to do research in Canada, to recruitment and retention of top scientists and to the evolution of research methods. The purpose of this project is to examine the effects of high impact health infrastructure investments on health research grant funding requirements in Canada. This project builds on work recently completed by CIHR that documented:
- The distribution of federal health research expenditures between infrastructure, human capital and direct research support (2004).1
- Health research expenditures by federal, provincial and not-for-profit agencies; and estimates of future health research funding requirements, based on the growth of health researchers in Canada since 1999-2000 (2006).2
This body of work has grown out of a concern by CIHR about the appropriate balance of support for each of the elements that are essential to Canada's research performance (infrastructure, human resources, research institutions and research funding). This concern was recently articulated by an international review panel that carried out a review of CIHR's performance during its first five years (2000 to 2005).
'Each investment in personnel or building infrastructure inevitably puts further demands on the CIHR operating grant budget. If all such streams of funding were coordinated this would provide a powerful expansion in capacity across the research sector in Canada. When not well matched, however, significant new demands on grant support cannot be met. Failure to align these funding streams at a federal level creates a serious risk that supply and demand in health research becomes dangerously unbalanced'.2
The results of this study are relevant to the recently released federal Science and Technology Strategy, which calls for government to improve value for money by '...ensuring the right balance in funding for researchers, direct and indirect costs of the research they perform, research infrastructure, and research networks'.3
Objectives
The objectives of the project were to develop an approach and, if feasible, initial estimates to understand the effects of high-cost, large impact infrastructure investments on the following areas:
- The nature of research plans by institutions that have received funding from Canada Foundation for Innovation (CFI) and Canada Research Chairs (CRC) and the implications of those plans for CIHR investments in future.
- Methods for forecasting the demand for funding to support researchers and projects that use new infrastructure being put into place.
As information on high impact infrastructure projects was collected, the focus of this project became centered on the second objective. While research plans are discussed in a summary of stakeholder interviews, the main thrust of the work is to understand the impacts on funding requirements, research grant costs and research performance.
Conceptual Framework: Definitions
High impact infrastructure projects are defined for this project as new buildings, research laboratories, platforms and equipment that have received CFI awards of at least $1 million. CFI awards provide 40% of project capital costs, with matching funds from institutions and provincial governments providing the remainder. High impact projects therefore have a total value of at least $2.5 million.
High Impact health infrastructure projects included in this report are CFI supported projects that have been designated as health sector by project leaders. Multidisciplinary projects that are believed to have a strong potential for health research are also included. The use of a $2.5 million value threshold eliminates many projects that replace existing infrastructure or support individual research programs. All high impact health infrastructure projects represent new health research capacity in Canada.
Research performance is defined as expenditure for research and development carried out by the higher education sector (HERD).4
Demand for health research is created by the desire to improve prevention, public health, health care and health systems. Increases in the demand for health research arise from changing demographics and lifestyle, rising costs of health care, globalization, scientific progress and technological change.iii
Funding requirements are the means by which Canadian society expresses effective demand for health research. Most health research produces public goods, which cannot be sold in markets and must be funded through government support for research. Examples from health research would be knowledge about the beneficial effects of lifestyle choices, or new surgical treatments in publicly-funded health care systems.
Funding pressures are defined as the annual value of funding required to support health research in Canada.
Project Scope and Methods
A total of 239 high impact health infrastructure projects (49.9% of all high impact infrastructure projects) iv were identified through a review of the CFI online database. Of these, 221 were identified as health sector projects in funding applications to CFI and an additional 18 multidisciplinary projects were considered to potentially have a strong health research component, based on project descriptions. These projects included 204 that received CFI awards in competitions between 1998 and 2005 and 35 projects that received funding awards in November 2006. Analyses of these projects included the following data sources:
- CFI project progress reports from 161 of the projects were aggregated by CFI for analysis. All projects are required to submit progress reports for the first five years after CFI funding is finalized, and the 161 projects included all those that had submitted progress reports in 2006 or 2005 (only 3 high impact projects did not submit reports; 19 others had completed their reporting cycles while 20 had not been finalized). Breakdowns of the data were provided by stage of completion for all 161 projects and by institution for a subset of 143 projects;
- Interviews were conducted with twelve VPs of research from institutions across Canada. Six high impact health project grant award holders provided comments and detailed information on their projects;
- The CIHR Funding database was queried to determine grant funding trends for institutions hosting high impact projects; and
- Special data analyses were provided by the University of British Columbia, which has 31 high impact health projects (13% of total high impact health projects). These analyses included dates of completion for each project and distributions of funding between the components of construction, equipment and renovation.
Investments in High Impact Health Infrastructure Projects
CFI provides funding to universities, hospitals and colleges for infrastructure projects. CFI awards are made through open competitions and include funding for facilities, major equipment, databases and research platforms. CFI awards cover 40% of project capital costs and the institutions that receive the awards and provincial governments funding the remaining 60%.
CFI awards to high impact health infrastructure projects, as defined in this report, total $1.178 billion, 39% of all CFI project awards up to the end of 2006.v The total value of high impact health infrastructure investments with matching funds from institutions and provincial governments is $2.946 billion.
Figure 1
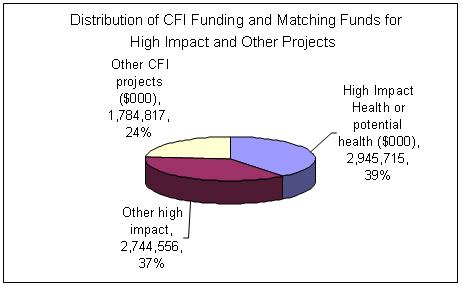
Source: CFI online database.
Many institutions have made additional investments in new construction financed by provincial governments, foundations and donors. Often, CFI project awards fund labs or diagnostic facilities within the new buildings. Several of the high impact projects at UBC, for example, are housed in a new life sciences building constructed with funding from the provincial government and donors. In Alberta, at least 7 high impact health projects at the University of Alberta are housed in the Health Research Innovation Facility (HRIF), a $165 million centre presently under construction. Construction of the new centre is being funded by the Government of Alberta, the Alberta Heritage Foundation for Medical Research and a fundraising campaign. 5
Time Required to Complete High Impact Health Projects
High impact projects often take many years to reach completion. Reasons include time required to negotiate matching funds, identification by host institutions of sites for labs and equipment and, in some cases, the construction of new buildings.
The pattern of high impact project approvals and completion dates at the University of British Columbia (which has the most CFI high impact projects) suggests that the major impacts of high impact projects awards since 1999 are just becoming evident and will increase over the next five years (Figure 2). Although UBC has been a major recipient of high impact awards in all the CFI competitions to date, 2004 was the first year in which projects were competed. Most projects have completion dates between 2006 and 2008. Eight projects have not yet begun and completion dates are not known at this time.
By fiscal 2005-2006, the first year for projections of funding pressures in this report, projects valued at $56.3 million had been completed at UBC, representing 15% of the total value of $381 million for high impact health projects at UBC, including matching funds (Figure 3).
Figure 2
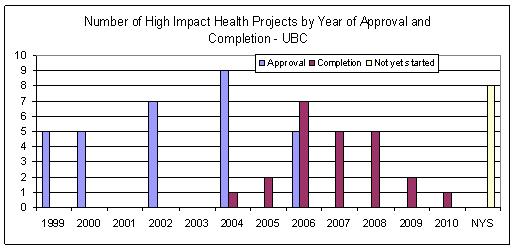
N.Y.S: Project not started and completion date unknown
Source: University of British Columbia
Figure 3
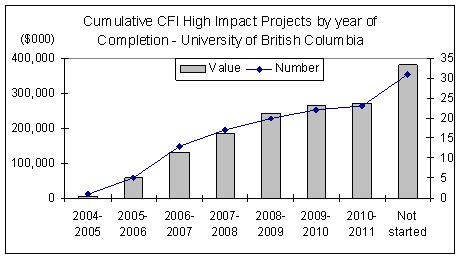
Value includes matching funds.
Source: University of British Columbia
Types of Expenditure for High Impact Projects
Expenditures for CFI awards are classified within the categories of (1) construction, (2) renovation, (3) equipment and other expenses. Most projects focus on equipment and, in many cases, renovation of premises to house new equipment. Construction awards tend to have higher average value, however. The distribution of funding for 31 high impact health projects at the University of British Columbia indicates 32% of total funding for construction and the remainder for equipment and renovations (Figure 4). Some projects include all three categories of expenditure.
Figure 4
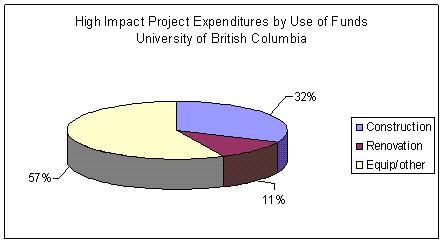
Source: University of British Columbia
![]()
Analysis of CFI project reports for high impact health projects
CFI obtains annual project progress reports for the first 5 years after project budgets and development plans are finalized (finalization can take a few years after approval in the case of large complex projects). Data were summarized by CFI from 161 high impact health or health related project progress reports for 2005-2006 (or 2004-2005 where 2006 reports were not available). The data were broken down by state of project completion. A subset of data were provided for each of 19 institutions that had at least 3 high impact projects for which project reports were available - 143 projects were included. The project reports are prepared by project leaders and reviewed by institutions prior to submission to CFI. For a more complete discussion of the annual progress reports, reporting cycles and data quality, see CFI progress report analyses for 2005 and 2006.6
State of Development - Ability to Support Research
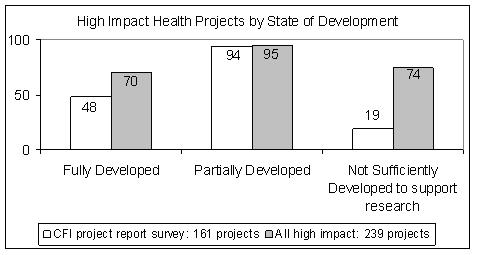
All project reports included data on state of development. Those data, supplemented by counts of projects that have completed their reporting cycle and projects that have not been finalized, are illustrated in Figure 5 (see notes to Figure 5 for a breakdown of projects not included in the 161 for which data were summarized). Approximately 71% of the 239 projects were only partially supporting research or were not sufficiently developed to support research during the year for which they reported.
The extent to which partial development reflects potential research capacity of a new facility is not reported and could vary considerably across projects. It seems reasonable to expect that there will be considerable increases in capacity to conduct research as these high impact projects are completed. One executive who was interviewed noted that it often will take about one year for a newly completed research facility to reach potential output.
Figure 5
Source: CFI Project Progress Reports
Notes:
- Partial development means that projects supported some research activities for at least part of the year. In some projects, equipment purchases are made over a period of time. Some equipment may be housed in temporary facilities pending construction or renovation of premises to house new labs.
- 48 projects in the project report survey were fully developed. An additional 19 had completed their reporting cycles before 2005 and three others were scheduled to complete their reporting cycles in 2005 but did not submit progress reports. These 22 projects were counted as having reached the fully developed stage in Figure 5.
- Projects not sufficiently developed to support research include 20 projects that had received awards between 2000 and 2005 but the awards had not been finalized, or had not been finalized long enough to require a progress report in 2006. An additional 35 high impact projects were approved by CFI in 2006.
Utilization and Funding Issues
This section examines the degree of utilization, useful years remaining and funding sources for high impact health infrastructure projects. Responses to most of the questions that are discussed in this section have been broken down between projects that were fully developed (48) and projects that were partially developed (94). An additional 19 projects were considered by project leaders to be not sufficiently developed (NSD) to support research. While some of the projects classified as NSD reported that they had attracted researchers, for the most part they were unable to report on utilization related variables.
Degree of Utilization
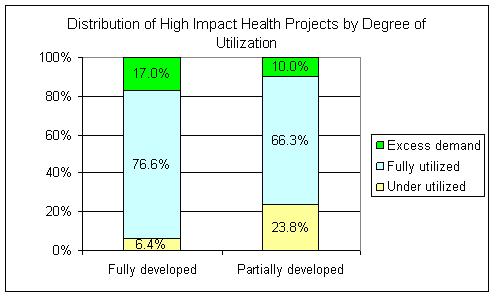
Over 93% of fully developed projects and 76% of partially developed projects reported full utilization of, or excess demand for, the infrastructure during the year reported (Figure 6). Of the 94 partially developed projects, 13 reported that the infrastructure was not sufficiently developed to judge the degree of utilization, 1 did not respond and 80 reported the degree of utilization. The percentages in Figure 6 are based on the 80 that reported the degree of utilization. Under utilization was more prevalent among projects that were partially developed. It seems reasonable to assume that the degree of utilization would be evaluated by project leaders in terms of the current state of development of infrastructure that is only partially developed. As a result, full utilization of a partially developed high impact project may not be a good indicator of the degree of utilization when development is complete. Full utilization throughout the useful life of a project will depend on a reliable stream of funding for operating costs, maintenance and research grants.
The degrees of utilization reported by fully and partially developed projects suggest that the infrastructure projects were wise investments in terms of scientific relevance as most new facilities contribute to Canada's research performance even before they are fully operational. Additional analyses of the data on degree of utilization would enhance understanding of the amount of research these projects will be able to produce in future, and the amount of funding that will be required to support research teams who will carry out that research.
Figure 6
Source: CFI Project Progress Reports
Note: 47 of the 48 fully developed projects and 80 of the 94 partially developed projects provided information on the degree of utilization. Projects not reporting indicated that infrastructure was not sufficiently developed to judge the degree of utilization.
Useful Years Remaining
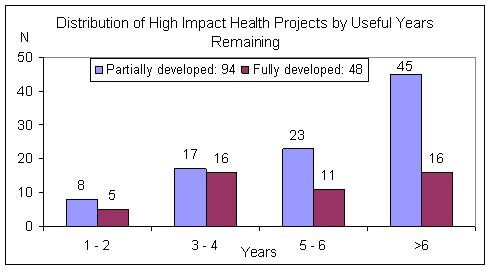
Approximately 48% (45) of partially developed projects have more than 6 useful years remaining, compared to only 33% (16) for fully developed projects (Figure 7). These data include both construction and equipment projects. Interviews with stakeholders indicated that, on average, new construction would have approximately 30 years of useful life while new equipment would have an average of 7 years. The useful lifespan for equipment varies. Certain technology is subject to very rapid pace of development, and obsolescence in terms of state-of-the-art research may occur in 2 to 3 years.
Figure 7
Source: CFI Project Progress Reports
Operating and Maintenance Funding
Funding for operating and maintenance (O&M) of infrastructure is a major concern in many high impact projects due to the relatively high costs of using and maintaining the infrastructure. Each item of highly complex equipment will normally require at least one technician. A PhD level scientist is required to achieve the full operating potential of some infrastructure, such as genomics platforms. Service contracts for maintenance of the equipment are also required and they were identified as a major item of expense by stakeholders interviewed. Responses to the project questionvi about access to operating funds indicate that approximately 28% of projects that were fully developed and 33% of projects that were partially developed had difficulty obtaining O&M funds (Table 1).
Table 1
Projects' Access to Operating and Maintenance Funds
| State of Development | Difficult | Reasonable | Responses | NSD or No Response |
| Fully developed | 13 | 34 | 47 | 1 |
| 27.7% | 72.3% | 100.0% | ||
| Partially developed | 29 | 59 | 88 | 6 |
| 33.0% | 67.0% | 100.0% |
Source: CFI Project Progress Reports
CFI has an Infrastructure Operating Fund (IOF), which provides up to 30% of the CFI capital award for operations and maintenance of projects funded under the Innovation Fund. The IOF funding is not available for projects approved before 2001 and it does not require matching funds. In effect the IOF provides up to 12% of total infrastructure cost for operating and maintenance. Almost half of partially developed projects reported that their institution had used funds from its allocation under the IOF to assist with O&M for the project. Only 30% of fully developed projects had received IOF funding (Table 2), likely reflecting a predominance of projects approved before 2001 in this category.
Table 2
Access to CFI Infrastructure Operating Funds
| State of Development | No | Yes | Responses | No Response |
| Fully developed | 33 | 14 | 47 | 1 |
| 70.2% | 29.8% | 100.0% | ||
| Partially developed | 44 | 47 | 91 | 3 |
| 48.4% | 51.6% | 100.0% |
Source: CFI Project Reports
A comparison of Tables 1 and 2 illustrates that many projects with reasonable access to O&M funding used sources other than CFI's IOF. Other sources would include university foundations endowments, research grants, user fees and contracts.
Impact on Major Sources of Funding
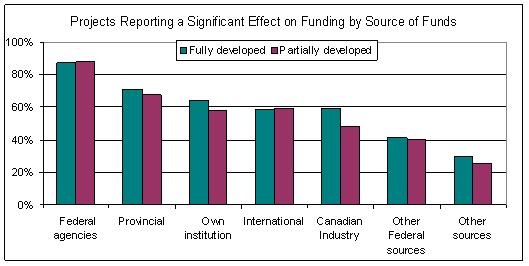
The project reports include the question, 'In the past year, has the infrastructure had an impact on the ability of its main users to attract new funds from the following sources?' Choices for each funding source include: no new funds, no impact, minor impact, significant or very significant impact. The percentages of respondents who reported a significant or very significant impact are reported in Figure 8. Approximately 88% of fully and partially developed projects reported significant impacts for federal granting agencies. Provincial sources ranked second. Researchers' own institutions and international sources ranked third with approximately the same percentage of responses. Funding by industry varied by state of completion, with 59% of fully developed projects reporting a significant impact compared to only 48% of partially developed projects.
The number of respondents for the six funding sources in Figure 8 varied by category. It's not clear if no response for a funding category could be considered equivalent to no funding from a source, since one of the choices for respondents is 'no new funds'. On the other hand, the varying number of respondents for specific sources suggests that in some cases a lack of response would be equivalent to no new funds. If we assumed that no response for a specific source meant no funding from that source the gradient in Figure 8 would be steeper. For example, 24 of 41 fully developed projects reported significant effects on funding from international sources. The percentage using 41 as a denominator is 58.5%. The 24 responses would be equivalent to 51% of all fully developed projects that responded to the funding question (47).
Figure 8
Source: CFI Progress Reports
Researchers and Technicians
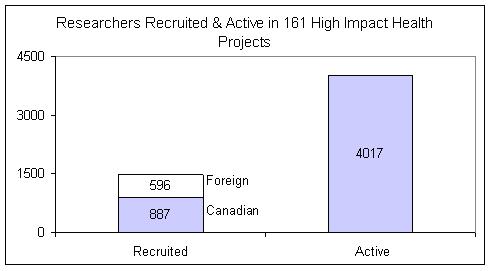
Projects in the sample reported 1,483 researchers recruited since the project began, 40% of whom were recruited from outside Canada (Figure 9). The average number recruited was 10.5 for the 150 projects that responded (11.4 for fully developed projects). The number of researchers participating in active projects was almost three times as great as the number recruited (Table 3). During the last year for which the projects reported, over 4,000 researchers reported advancing their research, approximately 70% of whom were from institutions other than the one in which the project is located. On average, there were 26.8 researchers per project.
The strong recruitment performance and the relatively large percentage of researchers from institutions outside the host institution (70% compared to 47% for all CFI project progress reports in 2006) likely reflects the quality of high impact health infrastructure projects. The progress reports ask project leaders to compare the quality of their infrastructure to other research facilities. Approximately 52% of fully developed projects, and 49.5% of partially developed projects that were sufficiently advanced to permit a comparison, were rated as comparable to the best in the world (considerably higher than the 37% rated best in the world in all project progress reports).
Table 3 also contains an estimate of technicians employed. This estimate, 1,674, is based on responses to a question about technicians trained on use or maintenance of project equipment and remaining at the institution. Respondents reported a total of 2,188 technicians trained since the project started. Technicians who were trained but have left the institution account for the difference between the two estimates. The estimate of 1,674 is a proxy for technicians required by the high impact projects, and probably a low estimate since there could be vacancies at some institutions in the required complement of technicians while others might employ technicians trained elsewhere. On average there were 12.6 technicians employed per fully developed project.
Figure 9
Source: CFI Progress Reports
Table 3
Health Researchers and Technicians - 161 High Impact Projects
| Researchers recruited since project began | Researchers in active projects last year | Technicians employed | ||||
| Canada | Other Countries | Total | Own Institution | Other Institution | Total | |
| 887 | 596 | 1,483 | 1,239 | 2,778 | 4,017 | 1,674 |
Source: CFI Project Reports
The average number of health researchers recruited was used to forecast funding requirements in Approach 1, which is discussed in a later section of this report. Results for each of the 19 institutions that had at least 3 high impact projects were used to test for variance in the mean values of researchers recruited. The standard deviation was 5.01 and the confidence interval for the mean number of researchers recruited was 7.9 to 13.2 at the 95% confidence level.
Discussion
The utilization and useful years of life profiles of high impact projects suggest that timely access to research funding is very important if these projects are to meet expectations from researchers and to achieve their potential contributions to research performance.
Utilization of new infrastructure projects in their early years may be partially supported by existing grants held by researchers who are recruited from other countries. Existing research grants normally will need to be replaced over one to four years, however. In the case of foreign researchers, it will be difficult to obtain support from granting agencies in their country of origin once they have relocated to Canada. Consequently, the amounts of international funding may decrease over time.
In the case of Canadian researchers, it is likely that they will have moved to new projects or research centres because of the potential to expand the scope of their research. For these researchers, new grants or grant renewals will often require higher levels of funding, especially if user fees are charged at the new facilities (the issue of user fees will be discussed more thoroughly in the section of this report that summarizes the results of interviews with stakeholders).
Researchers in high impact health projects report that the greatest impact of the projects on new funding occurs with the traditional sources, particularly federal and provincial granting agencies and the institutions that host the projects. Fully developed projects were more likely than partially developed projects to report significant impacts on funding from Canadian industry. This difference could signal a greater willingness of industry to invest in projects that are fully operational and/or have established track records. This issue deserves further research in view of public policy to encourage greater participation by the private sector in funding research.
![]()
CIHR Experience with High Impact Infrastructure Awards
British Columbia Cancer Research Centre
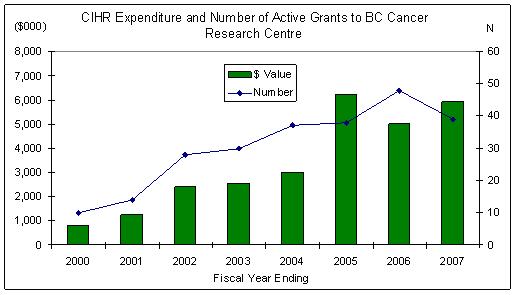
The British Columbia Cancer Research Centre (BCCRC) is one of the largest high impact health infrastructure projects completed and is fully operational. The BCCRC opened a new $95 million research centre in 2004. The CFI award to the BC Cancer Association for the establishment of BCCRC was $27 million. The new centre supports 'over 50 principal scientists and capacity for up to 600 scientific and medical personnel'.7
The number and value of CIHR grants to BCCRC increased substantially after the new centre opened (Figure 10). CIHR funding pressures in the last three years have averaged $6.1 million per year, almost triple the average of $2.2 million in the three years prior to 2003-2004.vii
The BCCRC receives substantial funding from the BC Cancer Research Foundation, other cancer not-for-profit agencies and philanthropy. Consequently it is not as dependent on CIHR for research funding as other health research centres. BCCRC reported that it received $56 million in research operating grant funding in fiscal 2005, equivalent to approximately 60% of the capital investment in BCCRC.
Figure 10
Sources: CIHR Funding Database and University of British Columbia.
Institutions with at least $15 million in CFI high impact awards
Nineteen institutions (see list in Appendix) received CFI high impact health infrastructure awards with a total value of at least $15 million between 1998 and 2005. These institutions accounted for 91% of the value of CFI high impact health awards during that time. Their share of high impact health awards in the latest CFI competition, announced in November 2006, was $135 million, or 81% of high impact health awards in that competition.
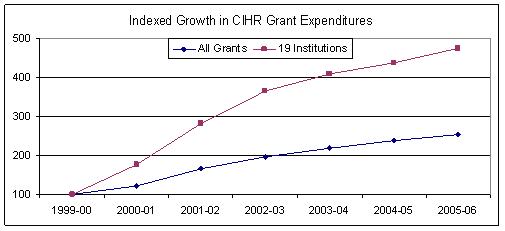
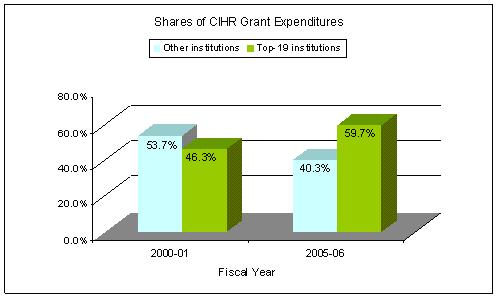
These institutions have increased their share of CIHR grant expenditures considerably since 2000-2001. Their indexed growth rates have been almost double the average growth rate of all CIHR grant funding (Figure 11). The 19 institutions accounted for approximately 46% of CIHR grant funding in 2000-2001 and approximately 60% in 2005-2006 (Figure 12). The extent to which there has been a cause and effect relationship between the CFI high impact awards and the higher than average share of CIHR grants is not clear. High impact infrastructure projects often take several years to develop and most of the impact of these projects on funding pressures from the 19 institutions will occur after 2005-2006. The success that these institutions have achieved with both CFI and CIHR probably indicates that most of the institutions have positioned themselves, through recruitment of researchers and planning strategies, to take advantage of opportunities for funding of both infrastructure and research grants. Fourteen of the nineteen are academic institutions and they have received 84% of the 551 CRC chair allocations in health that have been filled to date.
Figure 11
Source: CIHR Funding Database.
Figure 12
Source: CIHR Funding Database
Major Science Investments
Major science investments (MSI) are defined as 'those that are of sufficient magnitude that they exceed the capacity of a single institution, government department or agency to build and operate; they have scientific research as a primary objective; they have long-term financial responsibility or legacy issues; and there is a need to evaluate the non-scientific benefits.'8 Major science investments offer considerable potential to expand research and produce benefits for Canada and the scientific community - through innovation, commercial applications and direct economic impacts on the communities where they are situated. The Canadian Light Source (CLS) facility has been the largest MSI to be established in Canada in the last two decades.
CIHR provides $2 million annually toward the operating costs of the CLS. In addition to this dedicated funding, many researchers in the health sciences have expanded their research programs as a result of CLS, and they seek grant funding from CIHR in order to do so. CLS management advises that the first group of beam lines that will be mainly used in health research are presently being commissioned and others will come on line over the next five years. At present CIHR funded researchers account for approximately 11% of CLS usage; by 2012 this percentage is expected to increase to 25%.9
Canadian Light Source
The Canadian Light Source (CLS) synchotron at the University of Saskatchewan has been the largest recipient of CFI high impact infrastructure awards, with 9 awards totaling $100 million. (Three of the awards, including the initial award to establish the CLS, are included in the base of high impact health awards analyzed in this report.) Several academic institutions are participating in the development of CLS (3 universities received CFI awards to establish beamlines in November 2006). The CLS supports multidisciplinary research in the physical and health sciences. Total investment in the CLS to date has been $174 million, with additional investments of $64.5 million planned to establish additional beam lines (as of November, 2006).
The CLS facility consists of a central light source and several end stations or 'beam lines'. At present 7 beam lines are operational, although 5 are in a mixed-usage phase, with most of their available time used by CLS scientists who are commissioning the beam lines. All seven beam lines are expected to be available for open, peer reviewed access within the next year. By 2009-10, 14 beam lines are expected to be operational, with another 5 added in subsequent years. CLS began operations in October 2004 and is expected to remain operational for 40 years.
Access to CLS facilities is provided at no charge to academic and public sector researchers. All applications for access from these sectors must be peer reviewed in open competitions. Researchers are expected to obtain funding from the granting councils or other sources to complete the research projects for which beam time is required. Approximately 25% of the capacity on each beam line is available for use by the private sector on a fee-for-service basis. Fees are based on hourly rates for synchotron time and staff time. Although detailed cost and revenue breakdowns were not available, expected revenues from the private sector appear to be less than 25% of CLS operating costs. In effect, CLS provides a significant financial incentive to commercial users to carry out research at the facility.
The CLS has had an impressive record of expanding the capacity of the Canadian research community during its initial years of operation. There are approximately 16 synchotron related Chairs at the University of Saskatchewan and approximately 70 scientists at the university who use CLS facilities. Across Canada, 400 to 500 scientists use the facility. Over 2,000 user-visits per year are expected when the CLS is fully operational - a user-visit is defined as a period of time (usually 3 days) spent by a researcher at CLS carrying out experiments.
The largest source of funding for CLS operating costs is the NSERC Major Facilities Access (MSA) program. Annual amounts committed during the first funding cycle of CLS (ending in 2008-09) consist of $5.6 million from NSERC, $3 million from NRC and $2 million from CIHR.
Sources:
Dr. William Tomlinson, Executive Director, CLS
CLS website
CIHR and other funding partners provide dedicated funding to a number of other major initiatives for which CFI has provided infrastructure funding. These projects are generating or expected to generate major research activities (Table 4).
Table 4
Major Projects with Dedicated Operating Funding by CIHR and Partners
CFI & CIHR Clinical Research InitiativeCFI and CIHR have announced a joint initiative to invest in research hospital infrastructure and clinical research (January 2007). CFI is expected to commit $300 million to $350 million to infrastructure in a program titled Large Scale Institutional Endeavours and $100 million to infrastructure projects for the Clinical Research Initiative. These funds are being provided through CFI's Research Hospital Fund. CIHR will commit $50 million to fund research through the Clinical Research Initiative over 5 years. Additional funding is being sought from partner organizations. Infrastructure being planned under the Clinical Research Initiative will be able to support 12 to 20 teams or networks of researchers. Each team will require $3 million to $5 million per year to achieve its research potential. A conservative estimate of research activity would be 15 teams. These teams would require $225 million over a 5 year time horizon at the low estimate of $3 million annually per team or $375 million at $5 million per team. Sources: |
Structural Genomics ConsortiumThe Structural Genomics Consortium (SGC) operates from the University of Toronto in Canada, Oxford University, UK and Karolinska Institute, Stockholm. SGC is funded by an international consortium. Canadian funding groups include CIHR, Genome Canada, the Government of Ontario and CFI. Phase 2 funding requested for SGC between July 2007 and June 2011 totals $126.5 million from all sources. CIHR is contributing $2.5 million annually over the 4 year period. CFI provided a $7.2 million award in 2004. |
The Research Data Centres National Network: Canadian Initiative on Social Statistics (CISS)Research Data Centres (RDC) provide access for social science researchers to complex data sets of Statistics Canada. CFI provided a $5.4 million award in 2000 to establish RDC at the Université de Montréal. SSHRC and CIHR are providing a $6 million multi-year grant. Amounts provided during fiscal 2006-2007 - CIHR: $600,000; SSHRC: $800,000. RDC reports that by June 2006, 13 centres were operating in 40 universities. There were 1,400 researchers in the centres including 400 students. Sources: CFI, CIHR |
![]()
Summary of Interviews
Interviews were held with 12 senior stakeholders, most of whom were Vice Presidents of Research at universities or research hospitals. The first part of the interview covered general directions in health research, the effects of new high impact infrastructure and implications for research grant funding. The second part covered new infrastructure projects at the respondents' own institutions, with emphasis on the process of planning for infrastructure acquisition and use.
Research Directions
Dr. Pierre Chartrand, CIHR's Vice President of Research, expressed the view that new technology and research methods are leading to a collaborative model for researchers, in contrast to the individual competitive model that has been the norm in past. This new model requires an approach that integrates diverse professional skills in order to carry out research using complex platforms such as genomics, proteomics and modeling techniques that use mice or other non-human forms of life to understand human processes. Such research typically requires scientists from a number of different disciplines.
Other stakeholders agreed that new collaborative models were increasingly important. Research with stem cells was cited as an example: the work requires processing of stem cells, implantation and 'putting labels on cells'. This process requires multiple highly sophisticated teams.
New infrastructure has influenced collaborative projects using highly sophisticated equipment and complex techniques. Within networks of universities, affiliated teaching hospitals or research organizations, several sites often collaborate or share in major equipment acquisitions. Most of those interviewed agreed that certain types of research affect the way that other research is carried out. Developments such as genome sequencing and mouse models have led to new techniques and approaches in many areas of medical research. These developments have created an ability to approach problems differently. One executive cited an analogy to the advent of computers and the internet - methods change and knowledge can be acquired much faster. There was uncertainty about the potential outcomes of these trends, however. They could represent a breakthrough in research methods, but the payoffs may be 10 years or more away in areas such as genomics and proteomics research.
Observations from the interviews include the following opinions and insights.
- Levels of research activity are increasing across Canada at present. CFI and CRC programs have influenced this trend by enabling universities to increase faculty and add new research facilities. New faculty are more focused on high intensity research than was the case in past, reflecting their training and backgrounds. Planning and coordination within faculty departments have improved, due partially to the fact that new projects require a lot of coordination to be successful.
- We are now are in the era of 'big science'. Infrastructure has enabled and accelerated this development. Researchers must now become affiliated with a research group in order to participate in some areas of research, such as genomics and related areas. A system-wide approach is required to achieve results in high priority areas. But research focus and fashion also influence the types of research being carried out. Some scientists with different priorities may be 'left in the lurch' by these trends. On the other hand, most major discoveries have come from individuals pursuing their own lines of inquiry.
The effects of new infrastructure on the average cost of research grant proposals are expected to vary according to the infrastructure itself and institutional approaches to funding operating costs. Some new infrastructure allows universities to expand research activities and recruit new scientists within the existing model of research activities, without a major impact on costs. Other infrastructure will allow new types of research, which will entail higher costs due to the nature of the infrastructure or the need for multidisciplinary research teams.
User Fees and Operating Costs
Opinions on whether or not the average costs of research grant proposals will increase as a result of new research equipment and platforms tended to be influenced by the issue of user fees for researchers who use the facilities. At one end of the spectrum, it was maintained that all costs of infrastructure should be eligible as charges to research projects using the facilities. These would include a share of technicians' costs, fee for service charges based on animals used in experiments and the cost of upgrading or replacing infrastructure. In research hospitals where scientists' salaries are paid by the hospital rather than an affiliated university, there is a case for including a share of these salaries in research grants.
At present, most institutions seem to have taken a cautious attitude toward user fees. Many institutions charge user fees although in some cases they are charged only to users from outside the institution or research centre. Others reported that user fees were not the norm at present but they are being considered. Concerns were expressed that reliance on user fees could create prohibitive costs for some research projects, and one centre reported that user fees were only about one-third of actual operating costs. Another concern is that some types of user fees would not be acceptable to granting agencies. There was also a concern that higher average costs of research grant applications could adversely affect competitiveness in grant competitions.
Research grants are an important factor in funding infrastructure because they cover some operating costs directly and also because grants from the federal granting councils increase an academic institution's allocation of funding from the Indirect Costs Program. Without research operating grants, institutions must either subsidize research with funding from internal sources or maintain new infrastructure that is used below its potential. The limited time in which most new technology remains state-of-the art for research increases the urgency of resolving this problem.
Where user fees are not charged or are insufficient to cover operating costs, institutions tend to rely on endowments or foundations to cover operating costs. There usually is no process in place to generate income for future upgrades to, or replacement of, new infrastructure. In one case, a university executive reported that his university provided financial support for research infrastructure from internal funds. This practice had encountered resistance from those in the academic community who believed that there was an imbalance between support for research and academic programs.
Infrastructure operating costs were an important issue for most institutions. Operating and maintenance costs of high impact infrastructure often exceed the 30% provided under CFI's Infrastructure Operating Fund. The IOF is targeted to the first 3 to 5 years of infrastructure operation and is not ongoing. Examples were cited where annual costs for technicians' salaries and service contracts were equivalent to 10% or more of a project's capital costs. Inflation and competition for skilled personnel have increased operating costs more rapidly than was anticipated at the beginning of some projects. In the absence of ongoing funding for infrastructure operating costs, institutions will experience pressure to recover these costs from user fees and research operating grants.
Some of those interviewed stated that there were examples across the country of high cost infrastructure that was not being used to its full potential because research groups that were expecting to use it had not been able to secure research grants. The result, as one respondent pointed out, can be a situation where Canada might have the best infrastructure but its scientists lack funding to use the infrastructure to its potential. Another respondent said that under-utilization of new infrastructure due to an imbalance between infrastructure and research grant funding was a major issue across the country.
Planning and Budgeting for Infrastructure
The second part of the interview dealt with infrastructure acquisition in the respondents' institution. Issues included whether or not a requirement for new high impact infrastructure was identified within the context of a strategic plan, and the effects on planning processes of the CRC and CFI requirement for institutional research plans.
Research Planning
One group of teaching hospitals reported a well structured planning process led by a research office. Areas of research concentration were identified in a strategic planning process. Infrastructure projects are developed on the basis of strategic priorities. The proposal process includes identification of a project leader and development of the application details. The research office leads this process, and it typically takes 4 to 5 months to develop a proposal. There have been some cases where a scientist identified an infrastructure project and led the proposal development process, but this is rare and such projects have been relatively small.
Other institutions reported that individual researchers or groups come forward with proposals for new infrastructure to advance research in their areas. In some cases these proposals were required to be consistent with institutions' strategic plans. In other cases the planning process was less structured and research plans would be modified to accommodate strong proposals led by eminent scientists. This process was described by one respondent as a case of research plans being developed 'after the fact'. In this model universities attempt to recruit very good researchers and design research plans around their capabilities. One respondent reported that the CRC program and its requirements for research plans allowed the university to become more focused in its recruitment. More than one institution expressed the opinion that success in obtaining large infrastructure awards (and research grants) was largely dependent on the involvement of strong teams of scientists who have international reputations combined with collaboration among departments or research centres. It is worth noting that this approach seems to link two different cultures - the traditional investigator led approach to research and the planned collaborative approach that some observers believe is becoming the new paradigm in major research initiatives.
Financial Planning
CFI funding, which covers 40% of the capital cost of infrastructure projects approved through peer review, provides a powerful incentive for institutions to identify infrastructure priorities. A contribution of this magnitude also provides a strong leveraging effect in obtaining provincial contributions and other matching funds from donors, foundations and internal university sources. Provinces provide varying percentages of matching funds, but most are close to the average of 37% across Canada.10 The remainder is raised by institutions.
Almost all the institutions interviewed have made major investments in new buildings and health sciences centres with funding provided by provincial governments and philanthropy. One institution reported that financial arrangements for a new health sciences centre included a $100 million bond issue, with the institution assuming a long term lease on the premises. Building projects valued at over $100 million were reported in Quebec, Ontario, Alberta and British Columbia. New buildings often house both teaching and research facilities. New research hospitals have been built or are in various stages of completion.
There appears to be a trend for wealthy donors to make large contributions to universities and in some cases to also lead fund raising campaigns. Institutions often recognize these contributions by naming a building after the donor. Investments in new buildings often benefit from CFI funding, but most CFI awards are for laboratories or research centres within the new buildings. In some cases the awards have been obtained before the institution has completed raising funds for a building. CFI awards are not finalized, however, until all funding required to support the project has been secured.
Several institutions reported that they require an analysis of operating costs and the identification of sources of funding for operating costs as a condition of obtaining institutional support for the application to CFI. Institutions in Ontario noted that most research there is done in research hospitals or institutions affiliated with, but not funded by, universities. Many scientists in research hospitals are on salary, which the institution is required to fund. Access to funding from the Indirect Costs program is also an issue, since these funds are normally provided to academic institutions. Sharing of revenue from the Indirect Costs program is normally governed by formal agreements between research institutions and affiliated universities.11
As noted earlier, research grants are a key factor in funding operating costs of new research centres or labs. In a business model, grants would also be a financial measure of the research 'product' produced in labs or research centres. Academic institutions tend not to think in terms of a business model, but nonetheless research is a raison d'etre for creating these facilities and research grants are essential to carrying out research. Institutions were asked if they had estimated the annual value of grant funding or commercial revenue required to justify investments in new infrastructure; the answer in almost all cases was 'no'.
![]()
Projections of Grant Funding Pressures
Approach 1: Number of Recruits
Grant funding pressures are defined as the annual value of funding required to support health research in Canada. This section provides initial estimates of funding pressures from researchers recruited to high impact health infrastructure projects. Researchers recruited to these projects are expected to acquire research operating grants to fund research opportunities afforded by the availability of infrastructure or new research centres. Other researchers active with the projects may have existing grants and renewal or replacement of these grants would not necessarily represent increased funding pressures - although future grants might be more expensive as a result of the new infrastructure, as discussed in the previous section.
Researchers recruited since the beginning of the 161 high impact projects in the CFI project report summaries represent only about one-third of the number of researchers who used the projects in the most recent year to further their research (in addition to researchers, the projects reported approximately 7,400 post doctoral fellows and graduate students had used the project infrastructure since 2001). Researchers recruited to high impact health infrastructure projects represent approximately 45% of the total number of health researchers recruited to Canada by CFI supported infrastructure projects since 2001 (Table 5).viii The projection of funding pressures based on researchers recruited therefore can be seen as a base for projecting minimum requirements. Interviews with experts in health research revealed that:
- Researchers recruited to high impact projects are often internationally known experts, and in some cases their presence may be a factor in securing the CFI award.
- These researchers tend to have high success rates in grant competitions due to their records of success.
- Many researchers will have multiple awards each.
Table 5
Researchers Recruited to Canada by Infrastructure Projects
| Country of Origin | Total CFI 2006 | Estimated Health | High Impact Health |
| Canada | 4,950 | 1,980 | 887 |
| US & Other Countries | 3,150 | 1,260 | 596 |
| Total | 8,100 | 3,240 | 1,483 |
Source: CFI Project reports.
The estimated health share is based on 40% of the value of CFI awards allocated to the health sector (CFI analysis, 2005).
On average, 11.4 researchers per project had been recruited in the 48 fully developed projects for which CFI project report data were available, somewhat higher than the average of 10.5 in the response data from all 161 projects. The 11.4 estimate was used as a better indicator of recruitment at project maturity - although this estimate may be conservative in view of the fact that successful projects often would continue to attract new researchers throughout future years of operation. An assumption was made that new recruits would all require research grants either on joining the institution hosting an infrastructure project or on completion of any existing grants that they might have brought to their new institution or research centre.
Average grant size was determined from experience with the 19 institutions that had received at least $15 million in CFI high impact health projects. These institutions together had 3,100 CIHR operating grants in fiscal 2005-2006. Experts at CIHR and other stakeholders who were interviewed agreed that average research project cost would increase as a result of the new infrastructure. Higher research costs will occur when using complex infrastructure that has relatively high operating costs and incorporates teams of researchers, such as genomics and proteomics platforms. It is difficult to assess the full effects of high impact infrastructure on the average costs of research grants, however, since many of the projects are only partially developed. Most of the partially developed projects, and some of the fully developed ones, were approved since 2001 and would be eligible for CFI IOF support. This support is typically considered to provide O&M support for a 3 to 5 year project cycle and projects would need to find other sources of support thereafter. Older projects that are not eligible for IOF support, and mature projects which have depleted IOF funding, would be expected to experience the greatest pressures to fund O&M costs through research grants. These projects may also be the ones most likely to have drawn down funding from endowments or other internal sources.
For the reasons discussed above, even the most recent averages for the 19 institutions will probably understate future grant funding pressures. In these estimates, the average for the 19 institutions in fiscal 2006-2007 was used as a 2005-2006 starting point. This average was adjusted to the full amount approved by CIHR Governing Council after peer review. The resulting average was approximately $175,000. Average grant size for the 19 institutions has been increasing rapidly during the last three years, however, and their average grant size in commitments for 2007-2008 is $207,000, an increase of 18% over the previous year (based on 2,050 active grants presently in effect or approved).
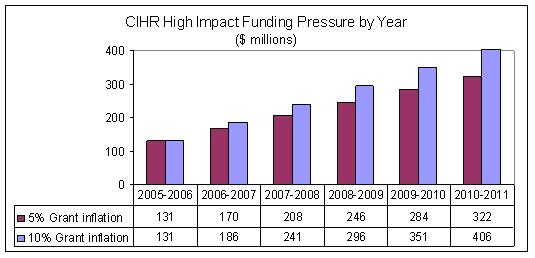
Two scenarios about inflation in grant costs were used to project requirements to 2010-2011, when all high impact projects approved to date were forecast to be fully developed. These scenarios each used straight-line increments in average funding pressure. Average grant costs for high impact projects were forecast to increase to $223,000 (equivalent to 5% per year) in the first scenario and $282,000 (equivalent to 10% per year) in the second scenario.ix
An assumption was also made that in 2005-2006 the extent of funding pressure from partially developed projects would be approximately 60% of the potential pressure at full development, while there would be no funding pressure in 2005-2006 from projects not sufficiently developed to support research.
The last assumption is that the share of funding pressures that will be expected to be absorbed by CIHR will be 54% of the total. This estimate is based on the CIHR share of total public sector and not-for-profit research grant funding in fiscal 2003-2004, analyzed in an earlier CIHR report.x These assumptions are summarized in Table 6. It is important to note that the assumptions are based on data available at this time, with future projections informed by expert opinion. The assumptions should be refined as time goes on, and as more data become available from specific high impact projects.
The estimates using approach 1 show high impact health infrastructure funding pressures totaling approximately $243 million in 2005-2006, of which $131 million is expected to be the responsibility of CIHR (Figure 13). The growth path of CIHR funding pressures to 2010-2011 indicate that funding pressure will be approximately $208 million to $241 million in fiscal 2007-2008 (Figure 14).
Table 6
Summary of Assumptions in Approach 1
| Average number of researchers recruited per project | All 10.52 |
Fully developed 11.42 |
| Percent of recruits: Canada Other countries |
59.8% | |
| Ratio of grants to researchers: |
1:1 | |
| Average annual value per grant (2005-06) |
$175,050 | |
| Grant inflation Scenario 1: Scenario 2: |
5% per year | |
| Weighted impact of funding pressures of projects partially developed and not sufficiently developed to support research: 2005-2006 2010-2011 |
P 60% 100% |
nsd 0% 100% |
| CIHR share of grant funding |
54% | |
Figure 13
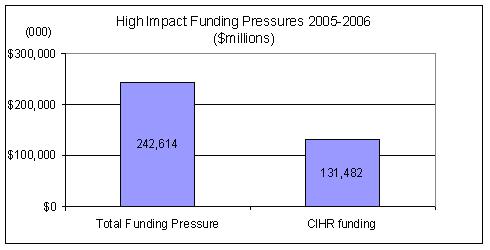
Figure 14
Discussion
Approach 1 combines quantitative data analysis of the effect of high impact projects and qualitative opinion about the interpretation of present trends and the nature of changes that can be expected in average grant cost. Both approaches indicate that the Canadian health research community has been strengthened considerably by high impact infrastructure that has recently been developed or is in the process of development. Anecdotal information suggests that researchers recruited to high impact projects tend to be scientists with a recognized track record or strong potential in the judgment of their peers. It seems reasonable to assume that these researchers will be in an advantageous position to obtain additional research funding to advance their work. This advantage arises from their recognized abilities, the opportunity to collaborate with others who are also associated with new research centres or initiatives, and the potential of the infrastructure itself to expand the boundaries of research possibilities.
The use of researchers recruited to high impact health infrastructure projects to forecast funding pressures is a conservative approach. Scientists who were at the host institution prior to the infrastructure award and collaborators from other institutions expect to expand the scope of their research programs through use of the infrastructure, and these enhanced research programs may have been the rationale for seeking the infrastructure award.
The average cost of research projects is increasing, as evidenced by experience with 19 institutions that have achieved above average records of success with both CFI and CIHR. Future costs are expected to increase, possibly quite rapidly, as new health infrastructure projects become fully operational and as mature projects become responsible for costs that are temporarily covered by CIF's IOF or by internal institution sources during their early years of operation.
Approach 2: Value of funded research Required to Justify Infrastructure Investments
Approach 2 uses an economic and financial planning approach to estimate the productivity of investments in high impact health infrastructure projects. Investments in infrastructure are viewed as potential contributions to multi-factor productivity, which includes the contributions of both labour and capital to growth in Canada's economic performance. Multifactor productivity is the preferred method of measuring productivity growth in areas where economic output is affected by technological change.12
The economic and financial planning criterion used in the approach maintains that:
Value added to research performance over the useful life of new infrastructure should equal or exceed the investment value of the infrastructure and associated costs of maintaining and using it.
Research performance refers to the value of research performed annually and reported by Statistics Canada as higher education research and development (HERD).13 The higher education sector is the largest of the five research performing sectors documented in a comprehensive series that tracks Canadian gross expenditures on research and development (GERD). HERD includes research activities by academic institutions and research hospitals. It consists of the following components:14
- The value of sponsored research.
- Indirect costs of research institutions.
- Value of faculty time.
- Indirect costs of faculty time.
In calculating value added to research performance by investments in high impact health research infrastructure we focus on the first component of HERD. Research activity is measured by the value of direct funding obtained for research projects. The other components of HERD, indirect costs and faculty salaries, are inputs into the research production process from institutions and scientists responsible for the research. The value of faculty time is not included as a cost associated with research using high impact infrastructure. Indirect costs are included only to the extent that they are associated with direct costs (item 2 above).xi
The investment value of infrastructure is a measure of the annualized value of replacement costs over the useful life of the infrastructure. It is calculated by the formula:
(amortization * inflation) - where amortization is the initial value of the infrastructure divided by its useful life. In these estimates, equipment and renovation expenditures are estimated to have a useful life of 7 years and new buildings (construction) to have a useful life of 30 years.
Annual costs of infrastructure include:
- Operating and maintenance costs of the infrastructure. The main elements are service contracts and salaries of technicians or scientists responsible for maintaining research platforms or high technology research facilities. Upgrades are also included, but not replacement of major components, which would require new applications for funding.
- Indirect costs associated with operating costs. The ratio of indirect costs to direct costs in HERD varies by university size. The ratio in large universities is .403.15 Ratios in medium and small universities are higher. An estimate of 40% was used for all high impact projects - most of which are located in large institutions.
The results of the methodology described above are shown in Table 7. Replacement costs for equipment and renovations are equivalent to 16% of the initial investment annually, over an estimated useful lifespan of 7 years. Replacement costs for new construction are equivalent to 6% per year, based on a useful lifespan of 30 years.
Operating costs are assumed to average 10% of the value of infrastructure. This estimate is consistent with examples cited by stakeholders interviewedxii, and is also consistent with operating costs cited in the report on major scientific investments by the National Science Advisor.7 The CFI Infrastructure Operating Fund assumes annual costs of 10% to 6% based on a 3 to 5 year operating cycle.
Table 7
Annual cost estimates for high impact health infrastructure
| Type of Investment | Share of high impact invest-ments | Value of Health Projects ($000) |
Replace-ment Costs ($000) | Annual Amortization | O & M Costs | Indirect costs | Total | ||
| Amount | Percent | ||||||||
| Equipment & renovations | 70% | 2,062,001 | 2,368,590 | 338,370 | 16.4% | 10% | 4% | 30.4% | |
| New Construction | 30% | 883,715 | 1,600,726 | 53,358 | 6.0% | 10% | 4% | 20.1% | |
| Composite | 2,945,715 | 3,969,317 | 10% | 4% | 27.3% | ||||
These estimates imply that the average annual costs of maintaining and using high impact infrastructure will be in the order of 27% of the capital investment. Consequently, the financial planning criterion used in this model would require average annual funded research equal to at least 27% of the infrastructure cost to ensure that the value of research made possible by new infrastructure is at least equivalent to the value of the infrastructure investment and operating costs. In practice, the value of research may be much higher. For example, in the B.C. Cancer Research Centre example discussed earlier, the value of research funding in fiscal 2005 was equivalent to almost 60% of the value of infrastructure investments.
These estimates imply that for every additional $1 billion invested in high impact health infrastructure, approximately $270 million should be invested in additional health research funding. This estimate is illustrated in Figure 15, showing the share that would be the responsibility of CIHR (54%) and the share that would be the responsibility of other sectors, if current patterns of funding were to continue.
Figure 15
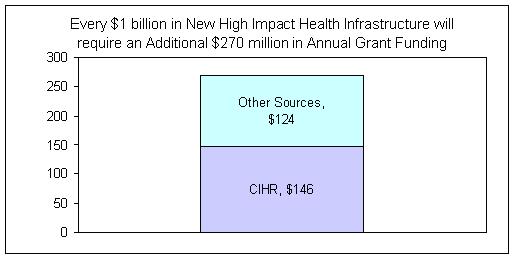
CIHR funding pressures are shown by year in Figure 16. Estimates of funding pressures in 2005-2006 were based on estimates of cumulative amounts disbursed by CFI for high impact health infrastructure projects relative to total commitments for these investments.xiii Ability to support research was assumed to be proportional to amounts disbursed (a simplifying assumption that is subject to an unknown degree of error). Progression from 2005-2006 estimates assumes equal increments each year to 2010-2011, when all project awards to date are assumed to have been completed.
These estimates indicate that funding pressures for CIHR from high impact health infrastructure projects would be in the area of $243 million in 2007-2008, increasing to $436 million in 2010-2011.
Figure 16
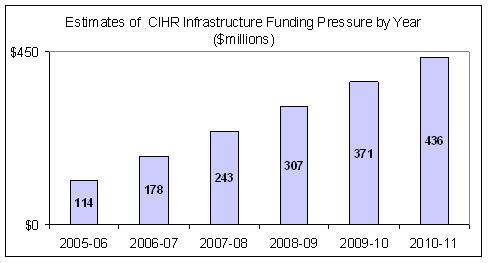
Comparison of Approaches
The two approaches to estimating funding pressures from high impact health infrastructure are conceptually different. The first approach estimates research grant funding pressure based on the number of researchers recruited to high impact health infrastructure projects. It is expected to be a low estimate since there is no additional funding pressure attributed to researchers at the host institution or at other institutions that also use the infrastructure. In addition, future funding pressures are subject to considerable uncertainty as a result of imprecise estimates of average grant costs using high impact infrastructure.
The second approach is based on a financial planning model. In effect, it mirrors a cost-benefit analysis that would be normal in private sector investments. The approach estimates future annual costs and calculates the value of research funding required to set benefits in the form of research performance equal to costs. These estimates are also subject to a relatively large degree of uncertainty. Successful infrastructure projects may attract considerably higher levels of research than the break-even levels estimated in the model.
Although the two approaches are very different in the way that estimates are derived, they both suggest similar orders of magnitude in terms of research grant funding pressures. Approach 1 indicates funding pressures for CIHR in 2007-2008 between $200 and $240 million. Approach 2 estimates $243 million. Differences between the two sets of estimates increase in future years, with funding pressures reaching $436 million in 2010-2011 in approach 2.
The estimates both assume a CIHR share of 54% of funding pressures. This percentage may be simplistic given the large increases in funding pressures and the relative budgets of CIHR and other agencies that fund health research.
Perhaps the largest uncertainty in both estimates is the amounts of funding pressure that agencies are actually able to satisfy. Funding pressures in the range of $400 million could potentially absorb 70% of CIHR's present grant funding budget, causing major distortions in other funding programs. Funding pressures of similar magnitude would almost equal the total grant funding budgets of all other public and NFP agencies combined in the 2003-04 estimates.
The straight line projections in both approaches do not imply that costs will continue to increase at the same rates once all high impact infrastructure is in place. It seems reasonable to assume a steady state situation in future in which successful infrastructure is upgraded or replaced to maintain state-of-the-art facilities. In that scenario, the 2010-2011 estimates could be seen as an indication of ongoing research requirements for high impact projects, to be adjusted for normal inflation - where 'normal' is defined in terms of the health research sector.
Lastly, these estimates are largely estimates of additional funding pressures for CIHR and other funding agencies. These agencies have seen a rapid expansion in demand for research during the last seven years. This demand has been driven in part by growing appreciation of the contributions of research to a knowledge based society and in part by major research advances that have created new potential. Funding requirements are the link between expressed need and effective demand for research. Agencies such as CIHR have long term mandates and strategies that will require funding even as new potential is created by advances in research methods and technology. As a result, the potential for substitution within existing budgets as a strategy to meet increasing funding pressures is limited, unless there is a willingness to abandon other worthwhile research.
If funding pressures cannot be met within future research budgets, the negative effects on Canada's research community could potentially offset the positive effects of investments in new infrastructure and human resource development during the first decade of the 21st century. In the most predictable scenario, scientists who have been attracted to Canada, or trained here at considerable public and personal cost, could migrate to other countries to pursue their careers.
![]()
Conclusions
Investments in research capacity during the last decade, in the form of human capital and infrastructure, have created a greatly enhanced capacity to do research in Canada. These increases in capacity have occurred at the same time as an increase in the demand for health research, caused largely by increasing awareness of the potential for health research to address some of society's most pressing challenges, and the recognition within the health sector of the importance of evidence based health care.
This report constitutes an attempt to assemble factual data and insight from experts in the research community that will help to understand present and future funding pressures from new high impact infrastructure. An understanding of health research funding pressures from high impact projects constitutes a major challenge for CIHR and for governments that understandably wish to achieve the most productive use of infrastructure to which public funds have been committed. Conclusions from this work are summarized below.
- New infrastructure is enabling major changes in the type of research that is possible and the ways that research is carried out. Multidisciplinary teams are expanding the scope and sophistication of research using complex platforms. System wide approaches are being used, such as the evolution from molecular biology to systems biology. Some projects have created large research centres that have considerable potential to position Canada's as a leader in health research.
- Canada's health research community has expanded rapidly as the result of several factors: high quality infrastructure funded by CFI and its provincial and institutional partners; programs to support scientists such at the Canada Research Chairs and career development awards; programs developed by CIHR and other agencies, and, in the early years of the decade, increasing research budgets. The separate and combined effects of these initiatives have not been well understood, but there is a growing concern about an imbalance between programs that fund capacity development and funding for health research.
- Funding pressures from high impact infrastructure projects have a lagged effect, since it may be several years from the commitment of infrastructure funding to the completion of the projects. The major impact on funding pressures has become evident in the last two to three years and will continue to grow until the end of the decade.
- Nineteen institutions have achieved quite extraordinary success in expanding their health research performance, accounting for over 90% of the value of high impact infrastructure investments and increasing their shares of CIHR funding from 46% to 60% in the last five years.
- High impact infrastructure projects have been successful in attracting health researchers from other institutions in Canada and from other countries. CFI project reports indicate that over 1,400 have been recruited to high impact infrastructure projects and over 3,200 have been recruited to all health infrastructure projects since 2001. The number of researchers reporting that their careers had been advanced by using the new infrastructure was much greater.
- The useful lifespan, before obsolesce, of high impact infrastructure is relatively short (approximately 7 years in the case of high technology equipment). Health research funding for scientists using new high technology equipment is a matter of some urgency if the equipment is to realize its research potential.
- The use of new infrastructure, combined with a multidisciplinary team approach, indicates that average annual research grant costs for projects using high impact infrastructure will increase rapidly
- The first set of estimates developed in this report is based on researchers recruited to projects that have reached full development. A second set of estimates is based on a financial planning model that maintains that the value of research produced in high impact infrastructure projects should be at least as great as the replacement cost of the infrastructure and its annual operating costs. While conceptually different, both sets of estimates indicate funding pressures for CIHR in the range of $200 million to $240 million in 2007-2008, possibly increasing to over $400 million by the first year of the next decade.
Appendix
Institutions with $15 million or more in CFI high impact health awards
University of British Columbia
B.C. Cancer Research Centre
University of Alberta
University of Calgary
University of Saskatchewan
University of Toronto
University Health Network
Hospital for Sick Children
Sunnybrook Health Sciences Centre
Mount Sinai Hospital
Queen's University
McMaster University
University of Western Ontario
University of Guelph
University of Ottawa
McGill University
Université de Montréal
Université Laval
Université du QC Institut national de la recherche scientifique
Note: The value of CFI awards in November 2006 was not included when selecting institutions with high impact health awards of $15 million or more
References
- Finding a Balance in Federal Health Research Funding. CIHR, Ottawa. September 2004.
- CIHR International Review Panel Report, 2000-2005 (Section 4, Risks). CIHR, June 2006.
- Mobilizing Science and Technology to Canada’s Advantage. Industry Canada, Ottawa. 2007.
- Estimation of research and development expenditures in the higher education sector, Catalogue number 88-001-XIE, Annual. Statistics Canada, Ottawa.
- http://www.cgi.ualberta.ca/hrif/index.php?page=cost
- 2006 Report on Results: An Analysis of Investments and Outcomes. Canada Foundation for Innovation. Ottawa, 2007.
- BC Cancer Research Centre
- A Framework for the Evaluation, Funding and Oversight of Canadian Major Science Investments. Office of the National Science Advisor, Ottawa. January 2005.
- Dr. William Tomlinson, Executive Director, CLS. Personal communication, March 2007.
- Alain Mallette, CFI. Personal communication, 2005.
- Glenn Brimacombe, Executive Director, Association of Canadian Academic Healthcare Organizations. Personal communication, January 2007.
- The Statistics Canada Productivity Program: Methodology 2000. Statistics Canada Catalogue no. 15-002-MIE (Page 6). Statistics Canada, Ottawa.
- Estimation of research and development expenditures in the higher education sector. Statistics Canada Catalogue 88-001-XIE. Annual. Statistics Canada, Ottawa.
- Estimation of research and development expenditures in the higher education sector, Detailed Information for 2004/2005. Science, Innovation and Electronic Information Division (SIEID), Science and Technology Surveys Section. Statistics Canada. Pdf: 5109_D1_T9_V2_E.
- Gisele Bellefeuille, Statistics Canada. Personal communication, Jan. 18, 2007.
Footnotes
- CIHR expenditures include flow-through funding for CRC, Networks of Centres of Excellence and Canada Graduate Scholarships (CIHR 2006, pg. 3).
- See Conceptual Framework below for a definition of demand for research.
- Demand for research is defined within a conceptual model described in the CIHR 2006 report (pgs. 19-21).
- There are 479 high impact projects across all research sectors, approximately 10% of the 4,862 projects that have received CFI support.
- CFI Project awards have totaled $2.99 billion, including the November 2006 awards. In addition, CFI has committed $516.2 million through the Infrastructure Operating Fund.
- The question is worded:’ In the past year, how easy or difficult has it been to obtain sufficient funds for Operations and Maintenance of your project?’
- Funding pressures include the annual value of CIHR grant expenditure plus the estimated value of grant applications that exceeded the peer review threshold for funding but could not be funded due to budget constraints.
- The numbers of recruits reported by the 161 high impact projects in the CFI project report summaries do not include 22 projects that had completed their 5 year CFI reporting cycle.
- The 5% and 10% rates of increase would yield estimates of average grant cost for high impact projects between $192,000 and $211,000 in 2007-08, compared to the actual average of $207,000 reported above. It is important to note that the estimates attempt to proxy the average cost of grants using high impact infrastructure, which would be expected to exceed average costs for all grants to the 19 institutions.
- CIHR 2006. Estimates prepared for the report were stratified by type of expenditure. The CIHR share of public and NFP sector research grant funding was 54.2%. An assumption was made that most private sector funding would go to product development rather than basic research, while basic research would be the main focus of high impact health infrastructure in its early years.
- Indirect costs are not normally an eligible expense in research grants by the federal granting agencies. The amount of funding obtained from the three granting agencies determines the shares that each institutions receive from the Indirect Costs program, however.
- In one example, basic operating costs for a $4 million MRI scanner consisted of a $190,000 for the salaries of two technicians and $210,000 for a service contract, summing to $400,000. A second estimate, for brain imaging equipment, indicated an annual cost of 10% for maintenance and at least that much in additional costs for personnel and supplies.
- CFI Annual Reports document total disbursements of $1.596 billion to the end of fiscal 2005-2006, of which $662 million are estimated to be for health sector projects. Health sector disbursements therefore represent 47% of total health sector commitments to the end of 2006. The estimates here assumed that 80% of awards less than $1 million would have been disbursed and consequently 38% of awards allocated to high impact health projects would have been disbursed.
- Date modified: