Internal Assessment for 2011 International Review - CIHR Institute of Health Services and Policy Research
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: The evolution of IHSPR strategic goals over time
- Figure 2: Percentage of total CIHR expenditures related to health services and policy research over time
- Figure 3: Specialization index and average of relative citations for top 10 countries publishing in access to appropriate care, 2000–2008
Mandate and Context
In the context of Canada's aging population, rapidly expanding technological possibilities, and increasing consumer demand and fiscal constraints, how should provincial governments decide which drugs to subsidize? What is the most cost-effective means by which they can improve access to primary and specialty health care? How should hospitals and long-term care homes improve the quality and safety of care they provide? How best can the federal government support the effective use of electronic health records? These are some vital questions addressed through the work of the CIHR Institute of Health Services and Policy Research (IHSPR). Established in 2000,
IHSPR supports outstanding health services and policy research and knowledge translation (KT) in order to contribute to improved health system outcomes.
In this report, we outline the initiatives IHSPR has undertaken to meet its mandate and achieve its goals. We also discuss key accomplishments in the 10 years of its existence, with a particular focus on the last five years. Our key messages are that IHSPR:
- is building a community of excellence and funds innovative and transformative health services and policy research (HSPR)
- develops novel funding tools that support the translation of research evidence into policy, and that are being built into the fabric of CIHR and emulated internationally
- leads and convenes opportunities to engender research that spans provincial boundaries and capitalizes on the natural experiments occurring across Canada's 13 provinces and territories
- has a dual role within CIHR as both an institute and leader for CIHR's overarching theme 3 (described below), thus supporting and encouraging HSPR externally with domestic and international partners as well as internally with CIHR's institutes and portfolios
IHSPR mandate: Support HSPR to improve health system outcomes
Our main goal is to support excellent research and its translation to inform decision making. We lead and convene support for strategic investments in research, KT, people and infrastructure within prioritized subject domains (e.g., access to appropriate care, pharmaceutical policy). We forge relationships with decision makers such as provincial deputy ministers and CEOs of health care organizations to identify policy-relevant research questions, and we partner with organizations such as Health Canada, the Canadian Patient Safety Institute, provincial research funding agencies and voluntary health organizations to leverage our funding and more effectively achieve our goals. Over the past 10 years, IHSPR, with the support of its partners, has significantly increased the size of the HSPR community, established research priorities relevant to decision makers' needs, and supported cutting-edge research that has directly informed policy-making and service-delivery improvements in areas such as wait times, patient-centred care, and health human resources.
The HSPR community has grown exponentially over the last decade. Unlike most of CIHR's other institutes, IHSPR does not have roots in CIHR's predecessor, the Medical Research Council. Although small hubs of internationally-recognized excellence in HSPR existed prior to CIHR's inception, the HSPR environment was underdeveloped. Accordingly, in its first five years, IHSPR focused on building an HSPR community, increasing the community's capacity to conduct excellent research, and forging partnerships to create more opportunities for researchers, interdisciplinary teams and training programs. For example, in 2000, IHSPR and the Canadian Health Services Research Foundation (CHSRF) partnered to support a 10-year, multi-program initiative in HSPR (the Capacity for Applied and Developmental Research and Evaluation in Health Services and Nursing program, or the CADRE program) that considerably bolstered capacity across the country with 83 postdoctoral awards, 12 mid-career chairs, five regional training centres and 13 career reorientation awards that have supported more than 1,250 researchers.Footnote 1 Although the HSPR community has developed considerably over the past 10 years, further growth is needed to address health system challenges and meet the need for HSPR evidence in Canada's health care system.
Over the past five years, IHSPR has continued to invest in building excellence while simultaneously prioritizing the need to support the translation of research directly into the hands of decision makers. To this end, IHSPR has helped CIHR become a leader in the creation of innovative programs that foster HSPR and accelerate its translation for evidence-informed decision making. With new programs such as Evidence on Tap and Partnerships for Health System Improvement, described in the Key Initiatives section, CIHR is increasingly regarded as an important resource for senior decision makers in Canada.
Our leadership in creating funding programs that directly support health systems decision making has also helped CIHR achieve its legislative mandate to translate new knowledge into a strengthened health care system.Footnote 2 Until the rapid response wait times initiative in 2005 and the Evidence on Tap program in 2008 (both designed by IHSPR), CIHR lacked a mechanism to meet its obligation to work in collaboration with the provinces and support health-policy decision making, as specified in the CIHR Act.2 As a result of IHSPR-led initiatives, provincial ministries of health now report that CIHR helps provinces achieve fundamental health system reform.Footnote 3
Characterizing IHSPR within CIHR and Canada
Several features distinguish IHSPR within the family of CIHR institutes and as a funder of HSPR in Canada.
First, in addition to its role as one of CIHR's 13 institutes, IHSPR is one of only two institutes (along with the Institute of Population and Public Health, or IPPH) that provide leadership for one of CIHR's four foundational research "themes". The CIHR Act categorizes health research into four themes, which all 13 institutes are required to support. The themes are: 1. biomedical; 2. clinical; 3. health systems and services; and 4. social, cultural, environmental and population health.Footnote 2 The aspiration at the inception of CIHR was that themes 3 and 4 would prove transformative, marking the transition from the old Medical Research Council (which was focused primarily on biomedical research) to the new CIHR, focused on multidisciplinary and translational research spanning traditional boundaries and disciplines, and leading to improved health services and systems. IHSPR leads, encourages and supports the 12 other institutes and portfolios to develop and support theme 3 research and researchers within their respective areas of focus (e.g., cancer and HSPR). IHSPR and IPPH operationalize their dual mandates – acting as institute and theme leaders – with the same staffing and budget as other institutes.
Second, the HSPR community in Canada was not well developed prior to IHSPR's establishment, there were few HSPR funders (e.g., the National Health Research and Development Program, which closed its doors in 1999, and CHSRF, which opened its doors in 1997), and the supporting infrastructure was limited. Therefore, IHSPR dedicated almost half of its annual budget and leveraged considerable support through partnerships to build research excellence. It did this through programs such as the Interdisciplinary Capacity Enhancement Teams, the Strategic Training Initiative in Health Research (STIHR), and New Emerging Teams. These investments have catalyzed growth in the HSPR community, as evidenced by the almost seven-fold increase in a decade in the number of researchers and trainees that identify as primarily affiliated with IHSPR.Footnote 4 CIHR expenditures related to HSPR have also steadily increased. However, according to CIHR data theme 3 continues to receive the lowest share of total CIHR expenditures compared to the three other themes.Footnote 4 Though the data have limitations (i.e., researchers may identify with more than one theme; the data are based on non-validated researcher self-selection; and a high proportion of researchers did not select any theme), they nevertheless speak to the need for IHSPR's resources and the importance of encouraging greater focus on theme 3 research by all CIHR institutes and portfolios.
Third, IHSPR oversees extraordinarily diverse, multidisciplinary and applied research that involves a range of subject matter and methodologies. Addressing health systems and services challenges – such as how to ensure appropriate diabetes care for First Nations in the North or how to reduce the rates of injury suffered by patients in home care – requires an interdisciplinary approach and the expertise of social and political scientists, economists, clinicians, epidemiologists, ethicists, decision makers and others. The heterogeneity of our field is a source of strength when different disciplines and methodologies can be harnessed to solve problems creatively; it is also a challenge, for example in peer review, when there is no common understanding of the range of methodologies or acceptance of the need for different metrics of excellence.
Fourth, IHSPR is the only national organization in Canada with an explicit mandate to support HSPR. Other organizations with which IHSPR frequently partners (e.g., CHSRF, Nova Scotia Health Research Foundation) have more specific mandates or are provincially oriented. At the national level, CHSRF's mandate includes supporting HSPR but in recent years its focus has shifted to supporting how decision makers use evidence, and to engaging citizens. At the provincial level, the members of the National Alliance of Provincial Health Research Organizations support HSPR but also support research in the other three themes (and with a provincial focus). IHSPR plays a vital role in the HSPR landscape by stimulating national approaches to complex challenges and by being the glue that binds a rich network of partners that support HSPR.
Canada's complex and changing health care context
IHSPR works to achieve its mandate within the constantly shifting landscape of the Canadian health care system. Canadian courts have said that the provinces have constitutional jurisdiction over the delivery of health care, which sets Canada apart internationally. The result is 10 distinct provincial health insurance plans, three territorial plans and three federal plans within the Canadian health care "system". The federal government contributes to the provincial and territorial health insurance plans through transfer payments and operates a number of health insurance plans through its provision of health care to First Nations and Inuit peoples, to the military and to prisoners. The federal government also regulates the safety of pharmaceuticals and is responsible for patent and immigration policy. This complex landscape has led to innovative provincial approaches for organizing and delivering health services (and valuable opportunities for natural experiments and comparative analysis), while also contributing to financial and geographical inequities in access to care.
In Canada, the growth of health care expenditures has outpaced growth in gross domestic product (GDP) since 1998,Footnote 5 and provincial health care expenditures threaten to exceed 50% of total provincial budgets within a few years.Footnote 6 These realities have spurred concerns about the long-term sustainability of the Canadian model. Policy makers and the public are also fearful that health care is crowding out spending on other important priorities such as education and social services. These trends provide impetus for a strong evidence base in HSPR and for cutting-edge research on how to adapt delivery models to emerging health challenges and opportunities such as chronic disease management and personalized medicine.
Institute Priorities
IHSPR pursues its mandate using two complementary sets of Institute priorities: the goals and objectives included within our strategic plan (e.g., building excellence, supporting KT), and the subject domains in which we make strategic investments (e.g., access to care, pharmaceutical policy). Strategic investments across these domains harness our $8.5 million annual budget and the support we leverage through partnerships. For example, we doubled our investment in our Applied Chairs Program from $3.2 million to almost $6.5 million through partnerships with six national organizations and we leveraged our $10.4 million investment in our Emerging Teams Program to $16 million with five partners.
To inform our strategic plan and our prioritized subject domains, we undertook extensive pan-Canadian consultations (e.g., the Listening for Direction exercise, described below, and a series of town hall meetings), worked closely with our Institute Advisory Board and expert sub-committees, consulted relevant literature and conducted environmental scans of HSPR priorities.
IHSPR's strategic plan
IHSPR has had three increasingly refined strategic plans since 2000. Figure 1 lists the goals of the Institute's second and current strategic plans. The key change between IHSPR's current strategic plan and its predecessors is streamlining. Having galvanized the community using an encompassing suite of goals in its earlier years, IHSPR now aspires to achieve greater impact with a more targeted set of four strategic goals. Figure 1 illustrates this evolution.
Figure 1: The evolution of IHSPR strategic goals over time
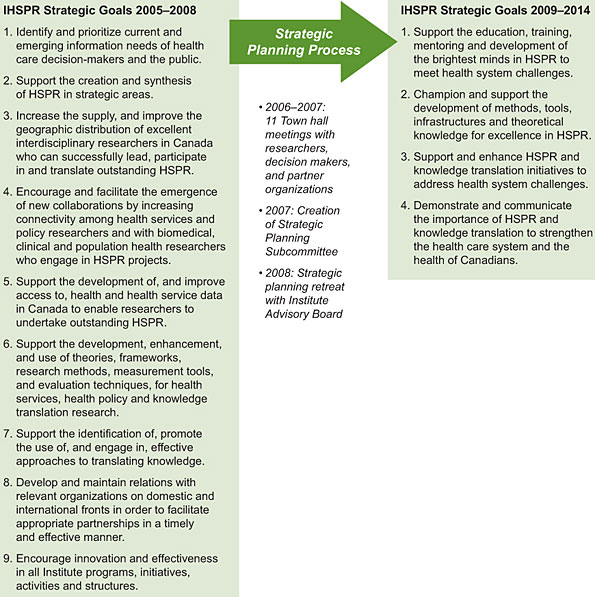
IHSPR's current strategic plan maintains our longstanding commitments – to support research, build capacity and transfer knowledge – but places greater prominence on supporting evidence-informed decision making. Additionally, the plan articulates a new goal of raising awareness within and outside CIHR of the value and importance of HSPR and KT to strengthen the health care system. This awareness raising is one of the ways in which IHSPR works to fulfill its dual responsibilities as an institute and theme 3 champion.
To complement IHSPR's 2009–2014 strategic plan we developed KT, international and evaluation strategies – useful frameworks for guiding the Institute's strategic and operational decisions and for assessing progress and measuring impact. IHSPR was the first CIHR institute to adopt a KT strategyFootnote 7 and appoint a KT officer, and other institutes have followed our lead.
IHSPR's prioritized subject domains
In addition to streamlining our strategic goals, we have reduced the number of subject domains (e.g., pharmaceutical policy) in which we target investments in order to increase our impact on HSPR and decision making.
For most of its existence, IHSPR has used the acclaimed Listening for Direction national consultation exercise to inform its prioritized subject domains.Footnote 8Footnote 9Footnote 10 Co-led by IHSPR and the Canadian Health Services Research Foundation (CHSRF) in partnership with other national agencies (e.g., Canadian Institute for Health Information, Statistics Canada), Listening for Direction was held in 2001, 2004 and 2007, each time involving six workshops across Canada and approximately 200 health system/service decision makers. In 2007, the consultations were extended to include Canada's three northern territories (Yukon, Northwest Territories and Nunavut), the outcome of which was a set of research priorities unique to the needs and challenges of Canada's North. Although today the involvement of decision makers in a research priority-setting process is common practice, in 2001, when Listening for Direction was established, the exercise was regarded as an innovation and catalyst in the field of applied HSPR. Between eight and 11 priority research themes were identified each year and IHSPR adopted all up to 2007; these are listed on IHSPR's website.Footnote 8
Post-2007, and informed by 11 town hall consultations with researchers and decision makers across Canada, our strategic investments are now guided by a smaller set of subject domains:
- access to appropriate care across the continuum (with a specific focus on community-based primary health care)
- pharmaceutical policy
- health information
- financing, sustainability and governance
These four domains reflect current and anticipated challenges confronting Canada's health care system. While some have been long-standing IHSPR priorities (e.g., access to appropriate care), others respond to newer challenges (e.g., using electronic health records to prevent and manage chronic disease) and anticipate future evidence needs (e.g., the needs of Canadian governments for evidence to inform their deliberations related to the expiration of the Health Accord in 2014). A full description of each subject domain is available on IHSPR's website.Footnote 11 The four domains also complement Health Research Roadmap, CIHR's new strategic plan, which provides opportunities for us to collaborate with other institutes, for example on our community-based primary health care strategy (see Going Forward).
Responding to CIHR's 2006 International Review
The 2006 International Review highlighted some of IHSPR's key strengths including its interdisciplinary focus, efforts to build capacity, responsiveness to decision makers, the theme 3 support it provided to CIHR and the strong leadership of then scientific director, Dr. Morris Barer. IHSPR has built upon these strengths and has also addressed the review's following recommendations for improvement:
-
To help "stabilize health services research capacity by filling the gap in salary funding between new investigators and Canada Research Chairs," IHSPR launched the Applied Chairs Program to support mid-career researchers who demonstrate excellence in research and in KT (see Key Initiatives).
-
To help "build the base for primary care knowledge generation," IHSPR allocated more than $3 million in 2009–2010 and 2010–2011 for primary health care research and is at present spearheading a flagship strategic initiative in this domain in partnership with CIHR and domestic and international organizations with planned investments of $50 million over seven years (see Outputs and Outcomes).
-
To "place more emphasis on the tracking and reporting of research products and impacts," IHSPR established an impact and evaluation subcommittee and hired a dedicated staff person to lead the Institute's evaluation activities.
The review also recommended that IHSPR "catalyze the development of academic centres for health services research." The situation for centres remains unstable as provincial government support waxes and wanes depending on economic fortunes. IHSPR's leadership in establishing the new Drug Safety and Effectiveness Network (DSEN), which has an annual budget of approximately $10 million,Footnote 12 will provide an injection of much-needed support for Canada's health services data research centres while also filling a critical research gap for Health Canada, provincial governments, health professionals and patients about the real-world safety and effectiveness of drugs. Additionally, in 2007 IHSPR partnered with CHSRF to provide an infrastructure grant to support the Network of 11 Centre Directors in HSPR from seven provinces to meet and share best practices. Going forward, it will be critical to monitor the health and vibrancy of HSPR centres across Canada.
Finally, the review recommended that IHSPR secure "additional resources at the CIHR level" to help with its "double duty." Although IHSPR has not received new unencumbered funding to help with its theme 3 leadership, we have secured additional multi-year funding from CIHR for specific HSPR initiatives, particularly those related to supporting innovative research and evidence-informed decision making. We have also worked closely with our institute partners to help them support HSPR within their mandates. For example, we invested with the Institute of Genetics to support a small but outstanding group of researchers in genetics and HSPRFootnote 13 (almost $10 million has been invested, primarily to support Emerging Teams and Operating Grants). Additionally, IHSPR has garnered significant external resources for HSPR (e.g., $10 million per year ongoing for the DSEN and 50% of the funding for the Applied Chairs).
Key Initiatives
This section discusses three key initiatives of IHSPR's and the activities that we have undertaken to support them. The key initiatives correspond with the strategic goals in our 2009–2014 strategic plan, and notable outcomes and impacts are highlighted in the Outputs and Outcomes section.
Initiative 1: Support the brightest minds to meet health system challenges
Building excellence has been a primary focus for IHSPR. With only a few organizations providing support for HSPR in Canada prior to IHSPR's establishment, we faced the challenge of building a vibrant community of researchers and supporting this community to achieve excellence in research and KT. Because academia continues to place greater weight on peer-reviewed publications than on applied research and KT, we also needed to recognize and reward the excellence and innovation of scholars committed to translating knowledge to decision makers. As an example of the problem we face it is salutary to note that there are just 22 PhD-trained health economists within economics departments in the top 10 universities across Canada.Footnote 14 Failure on the part of universities to value applied research results is a strangling of the potential supply of possible economics undergraduates interested in HSPR careers. To support the brightest minds in HSPR, IHSPR has led and partnered on a wide range of undertakings over the last decade that include the following:
-
The Institute has worked with partners to expand the HSPR infrastructure, which now includes the Canadian Association for Health Services and Policy Research (a national association for our research and research-user community with more than 350 members) and a peer-reviewed journal for HSPR called Healthcare Policy that is designed to meet decision makers' information needs.
-
IHSPR has built partnerships with organizations like the Ontario Ministry of Health and Long-term Care and the Victorian Order of Nurses to leverage additional support for HSPR and create linkages for researchers with decision makers (helping to ensure researchers are well poised to engage in effective KT).
-
The Institute has invested in multidisciplinary training programs, interdisciplinary teams, and salary and training awards for researchers and trainees that provide unique training experiences and help them to become strong competitors for other grants and awards.
-
IHSPR has supported the proliferation of pan-Canadian, interdisciplinary teams and networks conducting innovative research and harnessing the benefits of different provincial datasets and the natural experiments that emanate from varying provincial approaches to health reform, thus generating solutions to challenges that span provincial boundaries.
-
IHSPR has increased the availability of funding programs that support researchers and decision makers working together, that provide recognition for the value of applied research and its impact (e.g., CADRE Chairs), and that have appropriate peer-review metrics.
Initiative 2: Support the development of methods, tools, infrastructures and theoretical knowledge for excellence in HSPR
A high-performing health care system requires robust research grounded in state-of-the-art frameworks, methods and tools. In HSPR no gold standard method exists that everyone agrees upon; rather, in this multidisciplinary field, researchers utilize various approaches (e.g., quantitative, qualitative, mixed-methods). As a result, more time and education have been needed to understand the diverse approaches to HSPR and the value that diversity yields for improved health system outcomes. In addition, access to data is essential for innovative HSPR, which is why we committed in our 2009–2014 strategic plan to advocate for improved access to data and to facilitate best practices in data stewardship. To support excellence in HSPR, IHSPR has done the following:
-
With IPPH, we developed a novel funding program called Advancing Theoretical and Methodological Innovations in Health Research. Launched in 2002 and again in 2009, the program supports a combined total of 41 researchers to develop new theories, measures and frameworks for HSPR and population and public health research.
-
IHSPR hosted national summits such as the 2008 Health Information Summit (250 attendees and 12 partners) and the 2010 Primary Healthcare Summit (450 attendees and 18 partners) to unite researchers, decision makers, clinicians and partners from all four research themes to discuss the state of knowledge and future research directions.
-
The Institute provided leadership on behalf of CIHR in establishing the landmark DSEN, which provides much-needed infrastructure for drug safety and effectiveness research in Canada and is praised among international experts. Dr. Ruth Lopert (principal medical advisor, Therapeutic Goods Administration, Australia) reported, "better evidence of the real world risks and benefits of medicines is critical for sound decision making by regulators and funders, prescribers and patients. DSEN is an enviable model for driving research to address critical gaps in post-market data" (see Outputs and Outcomes).
-
IHSPR partnered with various institutes and organizations to improve access to research data for secondary use. IHSPR and the Ethics Office co-led the Compelling Values: Privacy, Access to Data and Health Research competition in 2003, which involved a number of partner organizations and privacy commissioners to support research related to the collection, use and disclosure of personal information for health research purposes. Also in 2003, IHSPR and 14 partners sponsored the Data, Data, Everywhere project and resulting report,Footnote 15 which was the first-ever national examination of the status and future potential of HSPR and population and public health databases in Canada. This project and the 2008 Health Information Summit raised awareness and catalyzed work with national and provincial partners.
Initiative 3: Support HSPR and KT to address health system challenges
Our goal is to generate excellent research that can be used to improve health system outcomes. Improvement can come about only if decision makers such as deputy ministers of health, regional health authority CEOs, and clinician leaders have timely access to high-quality research relevant to their evidence needs. IHSPR has thus made KT a central component of its work. We have accomplished the following:
-
The Institute has developed novel rapid research response programs such as the Best Brains Exchange (where we bring leading researchers and decision makers within provincial governments together for a one-day, in-camera exchange) and Expedited Knowledge Synthesis (where we support a synthesis on a priority topic for government in six months or less). These programs give decision makers access to outstanding research in areas they identify as top priority.
-
We have revitalized the Partnerships for Health System Improvement (PHSI) program, which catalyzes transformative research by linking researchers and decision makers throughout the research process. We have also made it easier for other institutes to become PHSI partners.
-
IHSPR has produced KT tools, resources and programs – such as CIHR's first-ever Casebook of KT success stories, the 2008 KT Summer Institute, the KT Strategy and the PHSI program – since emulated by other institutes and organizations inside and outside of Canada.
-
The Institute has engaged the public in evidence-informed dialogue through 10 HSPR-related Café Scientifiques on topics such as wait times, primary health care, and assisted suicide, and led a pan-Canadian Café series on mental health that involved all 13 institutes, the Communications Branch and the Mental Health Commission of Canada through 14 Cafés that were held in nine cities across the country.Footnote 16
Outputs and Outcomes
Capacity building
Our investments, coupled with our theme 3 leadership efforts to galvanize institutes and external partners to invest in HSPR, have contributed to a marked increase in the number of researchers and trainees conducting HSPR in Canada. One indicator of this growth is that the number of researchers and trainees that self-identify IHSPR as their primary institute affiliation has increased from 240 in 2000–2001 to 1,642 in 2009–2010.Footnote 4 Though the data have limitations (i.e., researchers may identify with more than one institute; the data are based on non-validated researcher self-selection; and a high proportion of researchers did not select any institute), they nevertheless clearly indicate a growing community of researchers and trainees.
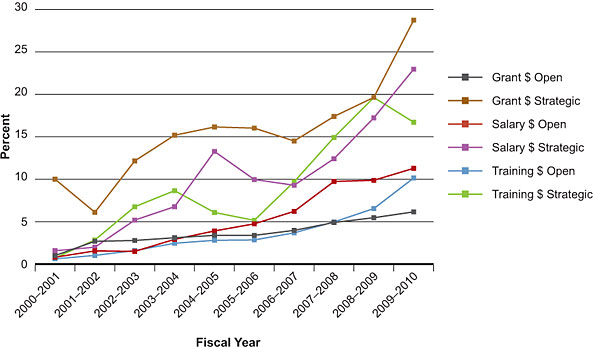
Another indicator of increasing research capacity is the consistently upward trend in the proportion to total CIHR expenditures in open and strategic funding for grants, salary awards and training awards in HSPR (Figure 2, based on validated data). Figure 2 also reveals that while HSPR's share of open competition funds has increased, it has done so more slowly than its rate of increase vis-à-vis strategic funds.
Strategic expenditures (from Institute budgets) have played an essential role in supporting health services and policy researchers and trainees since 2000–2001.
Figure 2: Percentage of total CIHR expenditures related to health services and policy research over time
While all institutes are mandated to support HSPR, CIHR data show IHSPR contributed the largest share to CIHR's total theme 3-related expenditures between 2000–2001 and 2008–2009 ($44.1 million, cumulatively).Footnote 17 The KT Branch is the next largest contributor ($17.9 million), followed by the Institute of Aboriginal Peoples' Health ($15.7 million) and the Institute of Population and Public Health, or IPPH ($15.2 million). Although institutes and portfolios have tended to increase their HSPR expenditures over time, there remains substantial room for growth. In future, we hope to see the fruits of IHSPR's more recent work to encourage stronger support for HSPR across all institutes (e.g., our 2010 HSPR Capacity Building Analysis and subsequent recommendations to institutes on how to better build excellence in HSPR).Footnote 18,Footnote 19 We also expect that our Community-based Primary Healthcare Strategy (see Going Forward) will galvanize institutes to build excellence in HSPR. Greater transparency and evaluation of each institute's investments in theme 3 will also enhance support for and growth in HSPR.
IHSPR investments and those of its partners in building excellence in HSPR have yielded positive outcomes for researchers and trainees in Canada. Selected examples are presented below.
Applied Chairs in HSPR
IHSPR launched the Applied Chairs Program in 2007 to support mid-career researchers dedicated to applied HSPR and to increase recognition within universities for excellence both in research and KT. With $3.2 million from six national partners (e.g., Saskatchewan Health Research Foundation, Health Canada), the program provides $6.5 million over five years for seven outstanding scholars who lead cutting-edge research programs and work in collaboration with decision makers on pressing health system challenges.
One of the researchers is Dr. Ivy Bourgeault (University of Ottawa), who received a CIHR New Investigator Award in 2001, does comparative research and conceptual modeling to improve health human resources planning, and works with officials from Health Canada on their Pan-Canadian Health Human Resources Strategy. She has leveraged her Applied Chair Award to secure an additional $1.3 million to study four countries' policy responses to migration of skilled health professionals.
Another one of the researchers, Dr. Michael Schull (Institute for Clinical and Evaluative Sciences, Toronto), works with decision makers from a ministry of health, the University Health Network, and a regional health authority to develop a scientific and policy-relevant program to improve access to quality care across the continuum. Dr. Schull received a CIHR New Investigator Award in 2001 and has since been a principal or co-investigator on more than $9 million in CIHR grants and awards. He was also recently awarded the prestigious Harkness Fellowship from the Commonwealth Fund.
Emerging Teams in HSPR
Since complex health system challenges often span provincial (and national) boundaries and require an interdisciplinary approach, IHSPR launched the Emerging Teams Program in 2007. The program invests $16 million ($10.4 million from IHSPR and $5.6 million from five partners) over five years to support 11 pan-Canadian emerging teams. The support enables researchers and decision makers from across the country and from different disciplines to work together and employ various provincial datasets to find solutions to a diverse range of complex challenges, and provide outstanding training environments for graduate students.
One of the teams is led by Dr. Steve Morgan (University of British Columbia) and works closely with Health Canada to develop new policies that will improve equity of access to medicines. With this support he leveraged a Commonwealth Fund grant to explore international expansion of some of his team's key activities. Dr. Morgan received a CIHR Fellowship Award in 2000–2001, a New Investigator Award in 2004–2005 and is a principal or co-investigator on more than $6.4 million in CIHR grants and awards.
"The emerging team funds enable hard-to-fund infrastructure and networking activities that translate into better research, KT and leverage for more opportunities."
Another team is led by Dr. Robyn Tamblyn (McGill University) and works with health informatic centres in Montreal, Ottawa and Boston to improve patient safety and chronic disease management with health information technologies. Her team is developing a hospital-based adverse events surveillance system and is testing whether electronic prescribing and interactive voice response systems improve pharmacosurveillance. Her team has leveraged funding from the Commonwealth Fund to study lessons learned from the Canadian and U.S. experiences with implementing health information technologies. She received a CIHR Investigator Award in 2000–2001 and holds or is a member of teams associated with $10.2 million in CIHR grants and awards.
Strategic Training Initiatives in Health Research
The 33 HSPR-related Strategic Training Initiatives in Health Research (STIHRs) in operation between 2001–2002 and 2008–2009 have attracted roughly 2,400 trainees who have benefited from innovative and multidisciplinary research training in diverse areas like primary health care, mental health services, medication safety and effectiveness, and health law, policy and ethics. Trainees receive invaluable mentorship and career-development support, gain exposure to cutting-edge HSPR methods and theories, and have the opportunity to interact with the foremost scholars and decision makers in their field. Trainees also publish and present with leading scholars (over a six-year period, each STIHR produced an average 96 publications and 296 presentations with trainees as lead or co-authorsFootnote 18) and establish relationships with fellow trainees through STIHR courses, Summer Institutes and workshops.
Rising Stars in HSPR
Thirteen rising stars have benefited from this award since we established it in 2008 to recognize research and KT excellence in early career stages. Recipients report that the award helped them secure postdoctoral and teaching positions and contributed to their success in other competitions, such as CIHR's New Investigator Award.Footnote 20 Their research is also garnering national attention through high-profile features in the Canadian news media. Dr. Mark-André Gagnon, a Rising Star Award recipient in 2010, was featured as an expert in a series of major news reports in September 2010 produced by The Globe and Mail, CBC TV News and other media outlets for his research on the economic gains Canada could accrue if it adopted a national public drug plan.Footnote 21,Footnote 22
Summer Institute
Since 2003, more than 250 trainees and 110 faculty from across the country have benefited from the IHSPR-IPPH annual Summer Institute, an innovative, multiday training initiative for top-ranked trainees.Footnote 23 The Summer Institutes are designed to strengthen capacity in applied and interdisciplinary HSPR and population and public health research. A survey of recent attendees found that more than two-thirds are still working in the field.Footnote 23 Students from the 2008 Summer Institute on KT have published in the journal of Implementation ScienceFootnote 24 and received a CIHR grant (Vivian Chan) to help establish a KT trainee community of practice. The perceived value of the Summer Institutes is evident in the tremendous support we have garnered from 18 decision-making organizations and 14 funding partners.
Advancing knowledge
Our goal is to invest strategically to build excellence in HSPR and generate new knowledge that advances the field and contributes to improved health system outcomes. A number of measures can illustrate the impact of IHSPR's contributions to advancing health services and policy knowledge. Specific examples of new knowledge created within HSPR programs and initiatives, bibliometric data related to IHSPR's prioritized subject domains, and total CIHR grant expenditures related to HSPR over time provide different lenses through which to view and understand that impact.
Examples of new knowledge created
IHSPR-funded researchers are at the forefront of breakthroughs in how HSPR is conducted and of new innovations in the science of HSPR. Their discoveries have catalyzed important shifts in the health care landscape in Canada (e.g., the establishment of provincial health quality councils and the Canadian Patient Safety Institute), and as scientific leaders (e.g., in KT science) they contribute to a global dialogue on HSPR. IHSPR has also made many direct contributions to the infrastructure that supports knowledge advancement. Examples include its $1 million investment in the Canadian Cochrane Network and its leadership to establish the Healthcare Policy journal. More examples that illustrate IHSPR's impact advancing knowledge in health services and policy are highlighted below.
Improving patient safety in Canada
IHSPR's partnership with IPPH, CIHR and the Canadian Institute for Health Information supported the first-ever study of adverse events in Canadian hospitals, led by Drs. Ross Baker and Peter Norton in 2002 – work that has transformed this area of research and informed policy change. The study found that roughly 7.5% of patients admitted to an acute care hospital experienced at least one adverse event of which 37% were preventable.Footnote 25 The study was first published in the Canadian Medical Association Journal and received significant media attention.Footnote 26 It is a widely-cited classic in patient safety researchFootnote 27 and has catalyzed patient safety improvements across the country. Indeed, not long after the study findings were released, the Canadian Patient Safety Institute was established. The study has also spurred research to improve patient safety in home care. In 2010, IHSPR and three other institutes partnered with the Canadian Patient Safety Institute, the Canadian Health Services Research Foundation (CHSRF) and the Change Foundation to invest $1.2 million into Canada's first-ever national study of patient safety in home care.
Public reporting in hospitals
Dr. Jack Tu won IHSPR's 2010 Article of the Year Award for his article called Effectiveness of Public Report Cards for Improving the Quality of Cardiac Care: The EFFECT study: A Randomized Trial. Supported by a $4.2 million CIHR Team Grant in cardiovascular outcomes research, the study, published in the Journal of the American Medical Association,Footnote 28 is the first randomized trial ever conducted to evaluate whether public report cards could improve quality of care. The study's methods and results have been used by hospitals across Ontario and other jurisdictions to improve their quality of care. As a result of his pioneering work, Dr. Tu has been invited to work with numerous other organizations in Canada interested in improving the quality of cardiac care. Dr. Tu presented his findings at the American Heart Association conference in 2009 where designated discussant Dr. Fred Masoudi (University of Colorado) stated, "...this is a landmark trial."
Advancing the science of HSPR and KT
IHSPR and IPPH's Advancing Theories, Frameworks, Methods and Measurements competition in 2002, highlighted in the Key Initiatives section, supported 29 projects (out of 104 applications) with an investment of almost $5 million ($2.2 million from IHSPR) and partnerships with two institutes and the CIHR Ethics Office. This investment fostered the creation of, for example, new theories to understand knowledge transfer (Réjean Landry), diabetes forecasting models (Jeffrey Johnson), computer simulation models to improve patient flow in surgical care (Boris Sobolev) and ethical frameworks for health policy (Nuala Kenny). We will closely monitor contributions to knowledge creation made by the 12 projects (out of 49 applications) recently funded in the 2009 competition.
IHSPR has supported research that advances knowledge about KT through a variety of mechanisms, including our $1 million investment over 10 years in the Canadian Cochrane Network, our more than $2.8 million investment over six years in research syntheses, and our support of leading researchers who improve our understanding about the science of successful KT. Renowned researchers France Légare (Laval University), Sharon Straus (St. Michael's Hospital) and John Lavis (McMaster University) have each benefited from more than $9 million in CIHR grants and awards and hold Canada Research Chairs in KT or a KT-related topic (e.g., implementation of shared decision making).
Bibliometric data
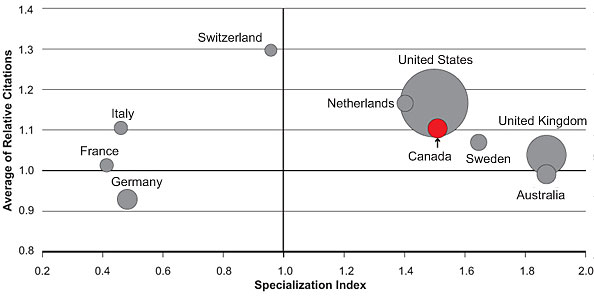
Bibliometric data are a second measure of IHSPR's impact on advancing knowledge. For example, CIHR's bibliometric analysis (informed by literature identified through Medical Subject Headings searches) examined Canada's ranking among the top 10 countries worldwide publishing in one of IHSPR's prioritized subject domains: access to appropriate care. The analysis used bibliometric indicators such as annual number of publications, annual specialization index (SI), which is the relative intensity of publications by country relative to the intensity of the world, and average of relative citations (ARC), which is the average number of citations received by papers over a two-year period following the publication year. The size and location of the bubbles in Figure 3 show that IHSPR's ARC and SI for publications in the area of access to appropriate care each rank fourth among the top 10 countries for 2000–2008 (1.11 and 1.51 for ARC and SI, respectively). Additionally, bibliometric data reveal that Canada was the third most productive country overall with 7,044 publications between 2000 and 2008.
Figure 3: Specialization index and average of relative citations for top 10 countries publishing in access to appropriate care, 2000–2008
CIHR expenditures
A final measure of advancing knowledge is the amount of total CIHR expenditures related to HSPR. Overall, grant expenditures related to HSPR have increased from $5.5 million in 2000–2001 to $97.5 million in 2009–2010 (open and strategic funding combined).Footnote 4
Strategic investments (i.e., from Institute expenditures) have been the major contributor to this growth.
Total strategic expenditures on HSPR-related grants increased from roughly $3 million in 2000–2001 to $69 million in 2009–2010. This represents a percentage increase of total CIHR strategic expenditures related to HSPR from 10% to 29%.
IHSPR's goal has always been that its strategic investments will help researchers and trainees develop increasing numbers of successful applications to the open competition. Over time, we have seen slow albeit steady growth in CIHR open expenditures on HSPR-related grants from approximately $2.5 million to $29 million between 2000–2001 and 2009–2010, which represents an increase from 1% to 6% of CIHR's total open expenditures (Figure 2). In future, greater attention must be paid to supporting and motivating IHSPR researchers to apply to open competitions.
The continued success and improvement of health services and policy researchers within CIHR's open competition depends on high-quality peer review. Peer review for HSPR remains a challenge. Moving forward, the Institute recognizes a critical need to improve the process so that outstanding HSPR is appropriately recognized. Careful attention is needed to organize review panels that will ensure excellence is supported across our field's wide range of disciplines and methodologies. This can be challenging given the size of Canada's HSPR community. When combined with the desire to eliminate relatively small peer-review panels, pressures being brought upon HSPR reviewers to understand and respect diverse methodological approaches may be aggravated. The Social Sciences and Humanities Research Council's recent devolution of health research from its mandate could bolster the size of CIHR's HSPR community though further exacerbate the peer-review challenges associated with such a multidisciplinary field. Innovative approaches (e.g., involving reviewers from other countries through information technologies) are required to ensure excellence in HSPR peer review.
Informing decision making
The vast majority of IHSPR's programs are designed to generate high-quality research and contribute to health services and policy decision making. Our two recent innovations in this domain are creating Evidence on Tap and transforming the Partnerships for Health Systems Improvement program.
Evidence on Tap
IHSPR developed Evidence on Tap in response to a need that decision makers have identified for timely research. Evidence on Tap comprises two distinct but complementary programs: Expedited Knowledge Synthesis (which produces a synthesis on a ministry-identified topic in six months or less) and Best Brains Exchange (one-day, in-camera exchanges between the "best brains" of the research and policy worlds that help government officials learn about the latest research evidence on a topic of their choice). These programs provide provincial and federal government officials with tailored and timely access to excellent research on topics that they identify.
Since Evidence on Tap was implemented as a pilot in 2008, IHSPR (with the support of the KT Branch) has worked closely with three provincial ministry partners to host 10 Best Brains Exchanges on diverse topics such as patient-centred care, managing surgical wait times, primary health care reform and more. The exchanges have involved 33 researchers and implementation/policy experts from Canada and abroad and more than 300 decision makers, including ministers of health, deputy ministers of health and finance, assistant deputy ministers and others. Evaluation data indicate that decision makers and researchers highly value our exchanges3 and, according to one of our Ministry partners,
"Now you hear our deputy talk about CIHR all the time. He talks about the Best Brains and says that what we're trying to do is accomplish fundamental change and that the Best Brains is helping us achieve this."
The Best Brains Exchanges have directly informed provincial decision making and program planning in areas such as wait times and health care financing. As just one example, IHSPR's inaugural exchange with Saskatchewan's Ministry of Health was on the topic of patient-centred care, which the ministry requested to help them prepare for the Patient First Review of its health care system.
According to Pauline Rousseau, an executive director at Saskatchewan Health, the exchange introduced the ministry to the concept of shared decision making, which has since become integrated into two province-wide policy initiatives.
Ms. Rousseau remarked, "We went from Best Brains to action really fast."
Partnerships for Health System Improvement
The Partnerships for Health System Improvement (PHSI) program has transformed the way health services research is conducted and has increased its impact potential by integrating decision makers as full-fledged members of the research team. IHSPR revitalized the program in 2008 by increasing funding levels, expanding topic eligibility, and to seed relationships between researchers and decision makers we created a new Partnership Development Funds competition. These efforts appear to have generated greater interest among researchers, decision makers and partners. For example, within CIHR, all but one institute now partners on PHSI and the program is being transitioned to the open suite of programs – a mark of success in embedding HSPR into the fabric of CIHR.
PHSI projects require external partner funding, which applicant teams are required to find. Partner support (cash and in-kind) is viewed as a concrete demonstration of commitment to the research; the sheer number and diversity of PHSI partners is evidence of the program's importance and vibrancy. More than 110 projects on diverse issues have been funded since the PHSI program's transition from CHSRF to CIHR in 2005. Projects include assessing models of care for individuals with mental illness, optimizing the practice of registered nurses within primary health care teams, improving priority-setting processes and more. Altogether, these projects represent a $5.6 million investment from IHSPR, which is leveraged to attract $28.4 million from more than 100 partners (internal and external) for a total investment of more than $34 million.
Persuaded by the success of our PHSI program, other countries such as Australia and New Zealand have followed our lead. Australia's National Health and Medical Research Council, for example, launched the Partnerships for Better Health program in 2008 to more effectively integrate evidence into health policy and service delivery.Footnote 29
PHSI research has informed decision making numerous times. The following are two of many possible examples.
In response to rising cancer drug costs and geographical variation in access to coverage, Dr. Peter Coyte (University of Toronto) and Dr. Roger Chafe (Memorial University of Newfoundland) are working with the presidents and vice-presidents of three provincial cancer agencies to understand factors that influence the adoption of new cancer drugs across provinces and institutions. Their research will inform the creation of a priority-setting toolkit for decision makers.
"This study will be, in my judgment, the first definitive characterization of the way drugs are evaluated and scheduled in Canada. It may also raise the possibility that we could press towards more of a common standard...as opposed to 13 different solutions to a very simple problem."
In response to serious concerns about the quality of care provided in long-term care facilities, Tim Burns (Ontario Ministry of Health) and Dr. Walter Wodchis (University of Toronto) worked with major stakeholders (e.g., the Ontario Long Term Care Association) to develop evidence-informed and practical solutions.
"This study is seminal. It has the potential to create groundbreaking cultural change within the long-term care sector. I can't say enough about what this type of research does for the health care system."
Health and health system/care system impacts
IHSPR's work has contributed to several notable health care system impacts, a selection of which are profiled below.
Informing wait time benchmarks
In 2004, first ministers committed to establish Canada's first-ever benchmarks for medically acceptable wait times in five priority areas by December 31, 2005. To ensure benchmarks would be informed by research evidence, IHSPR (under the leadership of its first scientific director, Dr. Morris Barer) spearheaded a rapid response funding opportunity called Toward Canadian Benchmarks for Health Services Wait Times and worked in partnership with Canada's provincial and territorial ministries of health and two institutes to fund eight research teams that synthesized national and international evidence on wait time benchmarks. Results were shared with ministries of health ahead of the December 31, 2005 deadline and are reported to have helped establish Canada's first-ever wait time benchmarks in cancer, joint replacement and sight restoration.Footnote 30
Improving the quality of neonatal care
With a $1 million Interdisciplinary Capacity Enhancement Team grant (2003–2007) in neonatal-perinatal care, Dr. Shoo Lee (University of Toronto) and his team have identified how health data can be utilized to improve quality of clinical care and reduce infections in neonatal intensive care units (NICUs). Using a new method devised by the team called evidence-based practice for improving quality (EPIQ), which combines the rigour of randomized controlled trials with the implementation strengths of continuous quality improvement, Dr. Lee and his team witnessed a 42% reduction in infection rates and a 15% reduction in chronic lung disease among pre-term infants in the 12 NICUs in their study, with an estimated cost savings of $70 million annually. Based on these results, the team received a PHSI grant in 2005–2006 to roll out the EPIQ method to neonatal intensive care units across the country.
Safe prescribing made simple
Dr. Robyn Tamblyn's computerized drug management system – the Medical Office of the 21st Century (MOXXI) – is improving the safety of drug prescribing for patients. MOXXI is designed to reduce human error in prescribing by giving physicians instant, computer-based access to a patient's drug, disease and allergy history, and by alerting physicians to potential prescribing problems. More than 200 physicians, nearly 80 pharmacies and more than 68,000 patients in Quebec are participating in MOXXI. CIHR's bibliometric analysis (described above) identified a 2001 article by Dr. Tamblyn on adverse drug-related events as one of the most frequently cited Canadian publications (n=280 citations).
Transformative effects
IHSPR, with the support of a rich network of partners, has played a pivotal role in transforming the HSPR enterprise in Canada. Although many challenges remain, this report has documented IHSPR's transformational effects in expanding a vibrant community of researchers who are conducting excellent research and addressing health system challenges; supporting cutting-edge research that advances the field and generates new theories, frameworks and tools for HSPR; creating innovative programs that other organizations are adopting; and galvanizing support among CIHR institutes and portfolios and, externally, among partners for investing in HSPR. In tandem, IHSPR is increasingly bringing transformational change to CIHR's funding programs.
IHSPR is leading CIHR's innovations to nurture HSPR. Building on its success with wait time benchmarks in 2005, IHSPR led CIHR in its provincial engagement strategy and developed the Evidence on Tap program. The program will expand from the pilot stage with three provincial partners to all 10 provinces and three territories in late 2010, which will herald a new era for the way in which CIHR engages with provincial policy makers. Additionally, the transfer of PHSI to CIHR's standing suite of open programs is further legitimizing applied and relevant HSPR within CIHR.
IHSPR's leadership in establishing the Drug Safety and Effectiveness Network (DSEN) further illustrates the Institute's transformative impact within CIHR, Canada and internationally. DSEN is by international standards a unique research program that fills a critical gap in the heath research and policy-making enterprise. Until its establishment in 2008, no organization had the mandate or capacity to do pan-Canadian post-market pharmaceutical research. High profile withdrawals of pharmaceutical products based on safety concerns (e.g., Vioxx) and the increased use of surrogate markers for market authorization purposes, among other factors, heightened the need for a pan-Canadian post-market research network that links provincial databases. IHSPR and Health Canada worked together to address this gap with the DSEN, which will build much-needed capacity for rapid and long-term research on the real-world safety and effectiveness of pharmaceuticals in priority areas identified by an expert panel of federal and provincial representatives, content experts, other agencies and a patient representative.
"Canadians can be confident that this government is taking the steps necessary to ensure that our drug safety system remains one of the best in the world. The Drug Safety and Effectiveness Network...results will help in decision making and enhance overall consumer safety."Footnote 31
Going Forward
IHSPR has made critical contributions to HSPR and KT excellence in Canada. Continued success and further advancements – so that CIHR can realize its full transformative potential as promised at its creation in 2000 – will require concerted efforts on several fronts, including:
-
A significant increase in the level of resources invested in theme 3 from across CIHR, as well as new investments from external (domestic and international) partnerships.
-
An increased focus on flagship strategic initiatives to galvanize CIHR and other partners, while maintaining core strategic programs open to a broader range of HSPR subject domains.
-
The timely seizure of opportunities to promote the benefits of HSPR and its relevance for and to federal, provincial and territorial governments.
-
Continued partnerships with CIHR's KT Branch to push the frontiers of programming at CIHR to deliver evidence to decision makers, as well as close collaboration with CHSRF to maximize synergies and position IHSPR to respond to changes in CHSRF's mandate.
More resources to achieve more impact and catalyze change
Since the advent of CIHR, the number of health services and policy researchers has increased seven-fold and the percentage of total CIHR expenditures dedicated to HSPR has tended to increase from year to year. Nevertheless, theme 3 has consistently received the lowest share of total CIHR funding when compared with CIHR's three other themes, which threatens to leave HSPR at the margins of CIHR's core business. From a global perspective, it has been said that insufficient resources are devoted to health systems research.Footnote 32 An opportunity exists for Canada and CIHR to increase its investments in HSPR, build on its many strengths and achievements, and capitalize on its natural potential (that derives in part from natural experiments occurring across 10 provincial, three territorial and various federal public health insurance plans) to be a world leader in HSPR.
A transformative agenda would see investments in HSPR steadily increase to ensure that the myriad of complex health system challenges facing Canada are tackled with robust research evidence. This would be money well spent given the returns from HSPR on improved health outcomes and cost savings (for example, the work of Dr. Shoo Lee discussed in Outputs and Outcomes indicates an almost 70-fold return on CIHR investment). Apart from providing the resources Canada needs to become a beacon for HSPR, increased investments would also enable Canada and CIHR to realize the many fruits of biomedical research through their successful translation into the health care system. Renewed attention to the possibilities of multidisciplinary work across CIHR's four themes of research would greatly enhance the translation of knowledge into clinical practice, service delivery improvements and policy.
Moving forward, strong institute leadership will be needed to meet these challenges and prospects (IHSPR's present scientific director, Dr. Colleen M. Flood, will transition in December 2010) and to forge new domestic and international partnerships that can substantially leverage resources for theme 3. Solutions are also needed on how best to galvanize support from CIHR's 12 other institutes and how, with current staffing and resources, to design theme 3 programs that have broad appeal (such as that achieved with PHSI). Continued leadership from the president and vice-presidents is also required to capitalize on the potential of HSPR both within CIHR and across Canada, for example in working with university leaders to promote the value of applied HSPR.
Flagship, transformative theme 3 research initiatives
As noted in the Institute Priorities section, IHSPR has increasingly streamlined the goals and objectives in its strategic plan and its subject matter domains. In the mid-term, IHSPR will focus on at least one flagship HSPR initiative, aiming to mobilize significant CIHR and partner investments, and with this achieve a major advance in knowledge and health care system impact. Historically, the average funding and duration for HSPR-related projects in the open competition have been small and short compared to those in biomedical and clinical research.Footnote 17 But the moment has come, given the HSPR research community and supporting infrastructure are now strong, to take a bold leap forward. CIHR's new strategic plan, Roadmap, contains an explicit priority to "support a high-quality, accessible and sustainable health care system" and this affords an invaluable opportunity to further galvanize support across CIHR for HSPR. As a consequence, IHSPR is developing a business case for CIHR and garnering domestic and international partnerships to support a community-based primary health care (CBPHC) flagship initiative.
The CBPHC initiative will build on IHSPR's previous investments and successes in the access to appropriate care prioritized subject domain. It was identified in 2009 as a top priority by IHSPR's Institute Advisory Board and in consultations with the HSPR. The initiative is explicitly designed to align with IHSPR's and CIHR's strategic plans. Four key factors make this an ideal time to launch a flagship pan-Canadian initiative in CBPHC:
-
Canada's 10 provinces and three territories are each implementing different versions of CBPHC, thus offering rich research opportunities.
-
Canada lags behind several other developed countries with respect to access, quality, comprehensiveness and coordination of care, and use of electronic medical records.Footnote 33,Footnote 34
-
Canada has pockets of excellence in CBPHC but has faced criticism for lagging behind in its commitment to primary health care research.Footnote 35
-
CIHR can lead a national research investment strategy, and evidence from abroad suggests that a concerted, coordinated effort can generate high-quality research and capacity that improves CBPHC.Footnote 36
CBPHC is intended as the first of a series of flagship programs centred on IHSPR's prioritized subject domains.
Seizing the moment and windows of opportunity
Canada's many health care systems are in a constant state of change, as are the needs and priorities of decision makers. IHSPR, with the support of CIHR, has responded quickly to windows of opportunity in the health care system, demonstrating to decision makers the value of research. Moving forward, IHSPR must continue to be ready, willing and able to respond to system needs as they arise. IHSPR will also need the continued support of CIHR and the other 12 institutes when a task dwarfs what is possible with IHSPR resources.
To this end, IHSPR and the KT Branch are leading on behalf of CIHR the Evidence-informed Healthcare Renewal (EIHR) strategic initiative. This $8 million investment over seven years will help CIHR meet its Roadmap commitment to "support a high-quality, accessible and sustainable health care system" by focusing on the financing, sustainability and governance of Canada's health care system. The initiative capitalizes on unique and time-sensitive windows of opportunity, including one presented by the upcoming expiration of the 2004 First Ministers' Health Accord, which set out the terms and conditions of transfer payments for health care from the federal government to provinces and territories. CIHR has the opportunity to mobilize research evidence that is responsive to government officials' evidence needs and convene KT opportunities that can contribute to evidence-informed decisions.
EIHR's first KT event took place in October 2010 as an invitational symposium for decision makers and researchers to discuss existing evidence, identify potential solutions and prioritize needs for future research. IHSPR partnered with the Nova Scotia Health Research Foundation, the Nova Scotia Department of Health (this year's lead province in the Health Accord negotiations) and CHSRF to host the symposium, which brought together 80 participants including deputy ministers and assistant deputy ministers in health, finance and inter-governmental affairs, high-level officials from across the country and leading researchers with expertise in health care renewal.
Our future role in providing evidence to decision makers
If a health care system were a body, information would be its blood. There remains an overwhelming need for information and research evidence to inform health system improvement and renewal – a reality true to all countries but particularly to Canada where many provinces now spend close to 50% of their budgets on health care. Economic and political pressures are enormous, exacerbated by the specter of an aging population, an influx of technologies frequently of marginal benefit and the perils and possibilities of personalized medicine. IHSPR will lead with other CIHR institutes and partners to offer Canadian decision makers the best possible evidence.
IHSPR's work will also be informed by the evolving role of CHSRF. For more than a decade, CHSRF has been a world-leader in bringing researchers and decision makers together to improve health services for Canadians. However, CHSRF's endowment ends in 2014. The organization released a new strategic plan in 2009, repositioning itself to no longer invest in the production of research and instead focusing on three priorities concerning the use of evidence: engaging and supporting citizens; accelerating evidence-informed change; and promoting policy dialogue. IHSPR will work closely with CHSRF to reconfigure and optimize its longstanding partnership in light of these new directions.
Over the last five years, IHSPR's work with the KT Branch to bring research into decision makers' hands has challenged old paradigms inside CIHR about what constitutes valid investment. It has also helped CIHR meet its mandate, in particular to provide support to provincial governments in the management of their respective health care systems. In future, IHSPR will continue to work with the KT Branch to push the frontiers of programming at CIHR and weave HSPR into the fabric of CIHR at all levels.
A final word
IHSPR will continue to support an outstanding community of health services and policy researchers producing cutting-edge research and translating that research into policy and practice. Recognized now as world leaders in specific pockets of HSPR –in KT, implementation science and patient safety – CIHR is poised to catalyze the HSPR community to be international leaders and grow the size of the community to better reflect research needs in Canadian health care systems. To nurture and sustain a world-class health care system – something that all Canadians strongly desire – we have to nurture innovation in the organization and management of those systems. To this end, IHSPR will continue to invest in people and the tools they need to conduct outstanding HSPR and KT; we will embrace transformative and innovative funding programs; and, in future, we will galvanize domestic and international partnerships for flagship initiatives of high strategic importance. With strong leadership, Canada will be an internationally recognized beacon for HSPR and KT.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IHSPR specific
| ARC | average of relative citations |
| CADRE | Capacity for Applied and Developmental Research and Evaluation |
| CBPHC | community-based primary health care |
| CHSRF | Canadian Health Services Research Foundation |
| DSEN | Drug Safety and Effectiveness Network |
| EIHR | Evidence-informed Healthcare Renewal |
| EPIQ | evidence-based practice for improving quality |
| GDP | gross domestic product |
| HSPR | health services and policy research |
| KT | knowledge translation |
| MOXXI | Medical Office of the 21st Century |
| NICU | neonatal intensive care units |
| PHSI | Partnerships for Health System Improvement |
| SI | specialization index |
| STIHR | Strategic Training Initiative in Health Research |
- Date modified: