Internal Assessment for 2011 International Review - CIHR Institute of Aboriginal Peoples' Health
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Advancing knowledge
- Building Indigenous health research capacity – A reflection of increased expertise and infrastructure
- Informing decision making through knowledge translation
- Improving models of good practice and health impacts
- Economic impacts of internal and external partnership investments
- Advancing knowledge in Aboriginal health and health research
- Transformative effects of the Institute
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures and Tables
- Figure 1: CIHR expenditures in IAPH mandate-relevant research
- Figure 2: CIHR funding for Aboriginal health research – percentage of total CIHR expenditures related to IAPH mandate areas over time
- Figure 3: Specialization index and average of relative citations for top 10 countries publishing in Aboriginal Health, 2000–2008
- Figure 4: Two-eyed seeing – A model for co-advancement
- Table 1: Number of publications, average of relative citations and specialization index across top 10 countries in Aboriginal health, 2000–2008
- Table 2: Number of community grants awarded by the nine NEAHRs from 2007–2010
Mandate and Context
The Canadian Institutes of Health Research (CIHR) Institute of Aboriginal Peoples' Health (IAPH) began conceptually in the summer of 1999. The Interim Governing Council of CIHR called for input on the nature and vision of potential institutes of health research. A group convened in Ottawa in 1999 that brought together academic researchers, Aboriginal nongovernmental organizations and government agencies interested in Aboriginal health research.
Though the group was small, it was apparent that these three sectors needed to work together to improve Aboriginal peoples' health. The option existed for an office of Aboriginal health contained within CIHR and aimed at influencing other institutes. However, given the unique and historical needs of Aboriginal peoples, including poor health status in comparison to non-Aboriginal Canadians and limited access to culturally safe and acceptable health services, the group believed a separate institute would better stimulate research interest, promote community engagement and increase research capacity. Viewed as necessary to reduce inequities and achieve significant improvements in the health of First Nations, Inuit and Métis (FNIM) peoples, the above three aims and the principle of self-determination became the key arguments for a stand-alone institute. Thus was born the CIHR Institute of Aboriginal Peoples' Health.
The Institute supports health research that addresses the special needs of Aboriginal peoples in Canada. The Institute aims to improve the health of First Nations, Inuit and Métis Peoples by:
- Leading a national, advanced research agenda that fosters innovative, community-based and scientifically excellent research
- Asserting Aboriginal understandings of health
- Enhancing knowledge translation and exchange
- Advancing capacity and infrastructure in FNIM communities
- Forging effective partnerships regionally, nationally and internationally
Health systems impacting Aboriginal peoples' health are complex and include federal, provincial, municipal and non-governmental bodies. Therefore, addressing the full mandate of CIHR requires each institute to resituate its own priorities within the framework of CIHR. The priority of CIHR to "reduce health inequities of Aboriginal peoples and other vulnerable populations",Footnote 1 suggests IAPH can expect to experience unique challenges with its enhanced leadership role in Canada's national Aboriginal health research agenda.
Challenges include developing and advancing initiatives and activities in keeping with CIHR's strategic directions:
- Invest in world-class research excellence
- Address health and health system research priorities
- Accelerate the capture of health and economic benefits of health research
- Achieve organizational excellence, foster ethics and demonstrate impact
Situating IAPH and its evolving priorities within the CIHR mandate "to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system"Footnote 1 demonstrates recognition at a national level of a need to seek marked improvements in the health of Canada's FNIM peoples.
Response to 2006 International Review
The Institute was praised for numerous advances and a recommendation was made for continued good practice. Areas noted as commendable included:
- efforts in research excellence, capacity development, funding strategic priorities in collaboration with other national Aboriginal organizations
- planning mechanisms
- approaches to consultation and relationship-building with Aboriginal communities
- efforts at knowledge creation, while recognizing a need to build capacity within Aboriginal and research communities to provide a foundation for increased knowledge creation in the future
- contributions to the transformative vision of CIHR through its emphasis on interdisciplinary research
Recommendations included increasing collaboration and partnering with national Aboriginal organizations, increasing the profile of IAPH, improving knowledge translation at the community level and improving performance monitoring. In response, the Institute has addressed each of the recommendations.
This has included a reordering of priorities to better align with the needs of communities and the development of standardized and acceptable "good" research and researcher practices. The mantra is "inclusiveness", "relevance" and "self-determination" of FNIM peoples.
The Institute has entered into new partnership agreements with Aboriginal organizations, and raised its profile through regional, national and international presentations and a range of print and online publications. Several performance measures have been undertaken, including an extensive impact evaluation and an inter-institute priority template. The development of the National Indigenous Database Tool (2009–present) also raised the IAPH profile, as did a national dialogue during 2009–2010: the Aboriginal Health Research Summits.
The Summits, carried out with FNIM communities across Canada, have and continue to inform the strategic priorities under development for 2011–2015. This dialogue has engaged more than 150 FNIM peoples across more than 10 disciplines (e.g., medicine, nursing, education, addictions treatment, health programming) to inform the future directions of IAPH. Fundamental underpinnings of the process included ensuring community and cultural practices and protocols encompassed the "ethics of practices." Inclusiveness was also exercised, helping to create a safe environment and facilitating recognition of community-level practitioners in improving the health and wellness of Aboriginal peoples.
Institute Priorities
- Develop strategic regional, national and international partnerships to advance Aboriginal health research.
- Ensure inclusion and recognition of Aboriginal values and cultures in health research.
- Enhance capacity and infrastructure to advance Aboriginal health research.
- Resolve critical Aboriginal health issues.
- Facilitate and evaluate translation of Aboriginal health knowledge into policy and practice.
The Institute utilizes several approaches to set priorities. These include:
- Institute Advisory Board biannual meetings
- collaborative initiatives with national Aboriginal organizations
- inter-institute collaborative research activities leading to the development of partnered funding opportunities
- tracking Institute reporting and evaluation initiatives to gauge the effectiveness and value of IAPH investments, in particular its major investment – the Network Environments for Aboriginal Health Research Program
Key Initiatives
The Institute has played a key role in identifying, articulating and translating the complexity of the underlying social conditions that impact the health of First Nations, Inuit and Métis (FNIM) communities.
Health problems within these communities are at extreme levels and include suicide, addictions, injuries, sexually transmitted infections and HIV/AIDS.
In addressing these problems, points of intersect between experts and communities have been identified as vital to achieving improved Aboriginal health.
Acting as the interface between health research, national and international health organizations, government and FNIM peoples, IAPH has led the advancement of a national health research agenda.
Advancements include recognition and legitimization of community-based research as a model of good practice for health research with Aboriginal peoples in Canada; this is a significant achievement of IAPH.
During the reporting period, IAPH focused energy and resources on the following key initiatives:
- Building Indigenous health research capacity
- Knowledge generation – Improving Indigenous health
- Leadership in Indigenous health research
Initiative 1: Building Indigenous health research capacity
To build Indigenous health-research capacity, IAPH focused on three strategies: community engagement, creation and support of a national Aboriginal health research network and development of ethics guidelines.
Community engagement
Fundamental to community engagement with FNIM peoples and to IAPH is the Aboriginal Capacity and Developmental Research Environments (ACADRE)-Network Environments for Aboriginal Health Research (NEAHR) program. The development, evolving structure and role of ACADRE-NEAHR, complemented by the Aboriginal Health Research Network and its Secretariat, continues to be critical to creating the structural support necessary to improve Aboriginal health.
Historical impacts on the health of Aboriginal Canadians are recognized as contributing to an underlying distrust on the part of FNIM peoples toward government, health and health care systems, research and other mainstream initiatives emanating from these structures. Colonization, assimilation policies, residential school legacies, economic and cultural marginalization and a long history of "fly-by, helicopter" approaches to research involving Aboriginal peoples have created and compounded this distrust.
By developing and supporting the ACADRE-NEAHR program, IAPH has fostered greater trust among FNIM communities and health research communities, which is conducive to improving health for Aboriginal peoples.
Strategies designed to engage communities in all facets of health research have been instrumental in this progress. Examples of engagement strategies include legitimizing community-based research and consulting with communities in the development of CIHR's Guidelines for Health Research Involving Aboriginal People.Footnote 2
The Aboriginal Health Research Summits process is a recent demonstration of an IAHP community engagement activity that helped navigate and advance a national Aboriginal health research agenda. This national dialogue facilitated knowledge exchange between IAPH and Aboriginal peoples and communities. It was mutually beneficial to all parties by engaging communities in the following ways:
- IAPH advanced the community's knowledge of the Institute.
- The community advanced IAPH's knowledge of critical health needs.
- The community advanced IAPH's knowledge by identifying research gaps.
- The community advanced IAPH's knowledge by assisting and guiding the Institute's vision.
Network Environments for Aboriginal Health
In 2001, IAPH responded to the limited Aboriginal health research capacity and expertise available across Canada by creating its flagship program: the ACADRE. Reviewed and enhanced since then, this program led to a new initiative in 2007: the NEAHR program. The primary objective of NEAHR's nine centres is to develop a supportive and advanced research environment in Aboriginal health across Canada. Key objectives include supporting students in Aboriginal health research, recruiting new and existing researchers in Aboriginal health research, engaging communities in research and promoting the rapid uptake of research findings for the improved health of Aboriginal peoples.
The NEAHR program has been instrumental in developing the capacity of Aboriginal health research and researchers. The program has also helped identify the health priorities and needs of Aboriginal communities, and informed and educated health workers and health research communities about issues paramount to improving the health of Aboriginal peoples. This includes developing accessible, specialized health research expertise in areas such as Aboriginal mental health and addictions. The Montreal NEAHR, the National Aboriginal Mental Health Network, support by IAPH in partnership with the Institute of Neurosciences, Mental Health and Addiction (INMHA), is an example. The ACADRE-NEAHR program embraces theme working groups in the following areas:
- Social determinants of health
- Ethics
- Health data
- Indigenous knowledge/traditional medicine
- Knowledge translation
- Mental health
Developing and supporting a growing cadre of Aboriginal health researchers and expertise, the ACADRE-NEAHR program supports networking and partnership activities between health researchers, research trainees and communities. For example, a 2010 NEAHR evaluationFootnote 3 reported knowledge and training of student researchers in the process of sharing research with other researchers as a real strength of the program.
During 2007–2010, the NEAHR program supported 336 student trainees through research grants.Footnote 3 In comparison, the 2001–2004 ACADRE program funded 125 students. Of these, 50% received undergraduate awards. Funding has now moved into primarily graduate-level awards: 11% of the 336 students receiving research grants are undergraduates, 41% master's students, 44% doctoral candidates, and 4% postdoctoral fellows (n=336).
The NEAHR program's focus is on highly accomplished students who demonstrate mentorship abilities, unique research topics and an ability to uncover new knowledge within the Canadian Aboriginal health field. "A student that represents the top third of NEAHR students had received three awards from 2008–2010, amounting to $27,420 that included a fellowship and two scholarships. This student also made six presentations from 2008–2009, all on Indigenous health including: healing, mental health, colonialism and policy".Footnote 3
Building on its position as the interface between community and Aboriginal health research, IAPH is currently renewing the NEAHR program.
NEAHR represents a network model of good practice in academic and community–research partnership and collaboration. As such, its successes demonstrate the extent of IAPH investment and the added value of the network to CIHR.
"The ACADRE-NEAHR process has been exceptional – Aboriginal communities and organizations are emerging as independent, autonomous and valued partners in the process of engaging in research that is relevant, meaningful and of value to the communities at large. The increasing pool of Aboriginal students and researchers engaged in Aboriginal health research independently or collaboratively with non-Aboriginal researchers has been a critical motivator for Aboriginal students and communities in viewing research as a potential future and career."Footnote 3
NEAHR's role in meeting long-term health outcomes
The activities of the NEAHR centres have as their long-term objective improving the health of FNIM Canadians. It is understood that the actions of the NEAHRs cannot directly affect long-term outcomes but that NEAHRs are instead part of the infrastructure that will eventually achieve long-term goals. The NEARHs fulfill an important role by identifying the critical health needs of communities and effect improvements in health outcomes for FNIM peoples by building research capacity, improving research quality, focusing on high-impact, high-need research and supporting the uptake of research evidence into policy and service delivery. The centres' key contributionsFootnote 3 include: improved research models and ethics in Indigenous research, training and capacity building for students and communities, and improved connections with researchers nationally and locally.
ACADRE-NEAHR has also made valuable contributions to the CIHR Guidelines for Health Research Involving Aboriginal PeopleFootnote 2 and the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans,Footnote 4 Chapter 9. These documents reflect significant advancements in knowledge translation and exchange between communities and researchers, and also reflect advancements in the development of health research capacity in areas of critical need.
Development of ethics guidelines
The Institute was created at a time when the Aboriginal health research environment was rife with bad practice. Improving ethical practice was recognized as an immediate need as well as an opportunity to foster trusting relationships with FNIM peoples.
The Institute is at the forefront of developing good ethics practice. It is recognized internationally as influencing ethics policy at the national level and was a key partner with the CIHR Ethics Office in the development of the CIHR Guidelines for Research Involving Aboriginal People.Footnote 2 This has moved CIHR into a position of moral leadership on a global scale. The ethics of good practice in Indigenous health research are now fundamental to the human dimension of all research.
The actions IAPH has taken to safeguard communities involved in health research have helped dissipate the mistrust that permeated FNIM peoples. Actions included collaborating on an ethics conference, which brought together academic researchers, ethicists and community leaders to discuss good and bad practice in Aboriginal health research. Another example is sponsorship of the Kahnawake Schools Diabetes Prevention Project as a model for good ethics practice. This project received CIHR's 2010 Partnership Award, the first formal recognition of a community partnership by CIHR.
The NEAHRs report three primary channels through which they apply ethics to research: CIHR guidelines used to review proposals for funding eligibility, a Tri-Council Policy Statement on research with humans implemented by institutional ethics review boards (REB), and development of community REB or community-based ethical protocols. Recognizing that the potential exists for Aboriginal peoples to contribute to their healing at a structural level, IAPH continues to play a significant and transformative role in the ethics of research with Aboriginal people.
Initiative 2: Knowledge generation – Improving Indigenous health
Knowledge generation, or those activities that form the foundations for knowledge translation and exchange, are at the heart of IAPH's core set of values and forward-moving vision. Beginning with development of Indigenous-specific research and academic scholarship expertise in fields and disciplines that impact health, IAPH has integrated into health research key principles articulated by Indigenous scholars. These principles relate to the significance of Indigenous cultures, values and Indigenous/community knowledge systems for the health and wellness of FNIM populations.
Expression of these principles in the development of Indigenous health and health research knowledge and exchange builds on the work of Indigenous scholars who have been the architects of Indigenous research methodologies and expertise. Pioneer documents, such as First Nations and Higher Education: The four R's – Respect, Relevance, Reciprocity, and ResponsibilityFootnote 5 and Aboriginal Knowledge Translation: Understanding and Respecting the Distinct Needs of Aboriginal Communities in ResearchFootnote 6 have impacted the development, activities and outcomes of research with Indigenous Peoples. In particular, the ethics of good practice in Aboriginal health research are alluded to in the works of Aboriginal scholars including Smylie et al.,Footnote 7 Weber-PillwaxFootnote 8 and Ermine.Footnote 9
Good practice is evident in a CIHR Team in Aboriginal Anti-diabetic Medicines, led by Dr. Pierre Haddad,Footnote 10 which addresses the devastating impact of type 2 diabetes (T2D) in Canadian Aboriginal populations. Wisdom from Aboriginal traditional knowledge has been made to cross-fertilize in a tangible, mutually respectful and efficient manner with that coming from modern biomedical sciences. This approach will allow the safe and efficacious use of traditional medicine by Cree diabetics who so desire. Results will also help develop novel factors that permit an effective early detection of T2D in at-risk sub-populations. The team has also developed an unprecedented comprehensive legal research agreement that goes to lengths previously unequalled to protect Cree traditional knowledge and related intellectual property.
On another front, Dr. Laura Arbour and team have established the Community Genetics Research Program, where conditions that affect Aboriginal people disproportionately are being addressed.Footnote 11 Current projects include:
- Primary Biliary Cirrhosis of the Pacific West Coast
- Long QT Syndrome in the North of British Columbia
- Biological and social determinants of birth defects in Nunavut
- CPT1A (Carnitine palmitoyltransferase type 1A) and its possible association with infant mortality in Northern aboriginal infants
A CIHR Institute of Genetics Clinician Investigatorship, awarded in 2003, and concurrent development of CIHR policy to protect Aboriginal communities in genetic research enabled establishment of the program.
Knowledge translation
Knowledge translation (KT) activities, based on principles of good research practice with FNIM peoples are key to ensuring that the benefits of health research are returned in usable forms to agency users, academic partners, policy developers and communities. IAPH has furthered knowledge generation in Aboriginal health and health research by engaging in activities that focus on knowledge translation and exchange, national partnership and funding initiatives and international partnerships.
Efforts in this area have focused on ways to develop partnerships and collaborations that may be applied effectively to KT. One outcome is development and sponsorship of a project that produced the 2009 brief Aboriginal knowledge translation: Understanding and Respecting the Distinct Needs of Aboriginal Communities in Research.Footnote 6 IAPH has also partnered with other institutes to support initiatives like the CIHR KT Branch Partnership Request for Applications. Current plans and activities of IAPH in the realm of KT include developing an Indigenous evaluation discussion paper and analyzing integrated KT in Aboriginal contexts. Recent findings of Smylie et al.Footnote 12 suggest participatory approaches can engage community partners in Indigenous knowledge translation research. Mainstream models of knowledge translation may be limited by their underlying assumptions in Indigenous contexts.
The NEAHR centres carry out coordinated and innovative approaches to knowledge translation, in addition to traditional academic-based approaches such as conference presentations and publications. Some examples include:
- distributing DVDs of community workshop proceedings
- making conferences available online and distributing them to communities, regional coordinators and researchers responsible for KT
- establishing an online health resource centre/information clearing house
- establishing networks with community health and political leadership, Aboriginal health practitioners, Aboriginal agencies and educators to facilitate information exchange
Dr. Judith Bartlett (Manitoba) is undertaking a study that implements and evaluates a novel knowledge translation model.Footnote 13 The study is grounded in a participatory action research approach, where each participation level has a specific goal, method and outcome for each of the research partners. This study is important to the federal government's Aboriginal Health Transition Strategy and acts as a guide for many other KT activities.
National and international activities aimed at knowledge generation
Institute strategies that support knowledge generation must link to knowledge transfer strategies that work at the community level. Creating space to recognize the "ownership" of community knowledge represents a melding of health research with community frames of reference and evaluation with validity. Developing and articulating these forms of engaged scholarship to bridge western and Indigenous views of knowledge indicates value for other ways of understanding, developing and using health. Such examples of "ethics of partnership," a foundational pillar of IAPH, increase the Institute's potential to mobilize community and researcher knowledge for the benefit of Aboriginal health.
Autonomy and self-determination are cornerstones of many Indigenous health philosophies. Aboriginal individuals' and communities' ownership of health can be seen as an expression of health and healing that has little to do with health policy. The complex and intricate relationships between culture, politics, economics and social justice may be broken down into concepts about healthy living and healthy dying. The fact that we now celebrate many Aboriginal people living to the age of 60 is a bleak demonstration of this issue. To improve the health of FNIM people, we must understand how this stream of knowledge informs immediate, action-oriented and sustainable research strategy.
Operationalizing these concepts at the national level has led to the development of funding opportunities in suicide prevention and resilience. Aboriginal health experts and communities have reported another innovative solution to health research needs: health intervention funding opportunities designed to support multidisciplinary, inter-institutional partnerships that develop and implement concrete, measurable intervention programs for critical FNIM health issues.
IAPH recently awarded four multi-year intervention research grants that will affect the social determinants of Aboriginal health. One brings together Aboriginal and non-Aboriginal scholars from Canada and the United States to take a poverty-reduction approach and thus improve the health and wellbeing of First Nations' communities in Canada. Led by Dr. Fred Wien and partnering with the Assembly of First Nations, the project draws on the experience of First Nations' communities in regions relatively successful in building a sustainable economic base and reducing poverty. It includes conducting a community needs assessment, contributing to the development and implementation of a strategic plan, and monitoring the intervention's impact over five years.
Initiative 3: Leadership in Indigenous health research
Since its inception, IAPH has been a leader in explicating the human dimensions of Indigenous health research.
Key impacts of this leadership role are:
- creation of international Indigenous health research partnerships and collaborations that have identified health research priorities for Indigenous Peoples at the international level
- creation of spaces and a forum for a continued dialogue of expertise in Indigenous health research at the senior academic level
- raising standards of scientific excellence in Indigenous health research
By investing in this multi-level approach, IAPH envisions changes at the senior international policy level influenced by international Indigenous scholarship and expertise. In light of formal apologies by the governments of Australia and Canada to Indigenous Peoples for the effects of egregious and harmful assimilation policies, IAPH's investments represent sound decision making. Legitimizing the voices of Indigenous Peoples increases potential to lessen their distrust of health research.
The Institute's leadership role in Indigenous health research is supported by unique methods and extensive, ongoing community engagement and consultations. Key Institute activities with regard to northern Canada's Aboriginal peoples include developing the Northern and Urban Aboriginal Strategy (2007), leading a partnership with CIHR in activities for International Polar Year, and holding a consultation session with northern health researchers at the 2009 14th International Congress on Circumpolar Health (ICCH).
The Institute has established and led numerous partnerships and relationships such as the International Network of Indigenous Health Knowledge and Development and ICCH, which have as a chief aim improving the health of Indigenous Peoples through combined efforts and learning in Indigenous health research. Additionally, a series of Indigenous Summer Research Institutes attended by experts in Indigenous health research from Australia, New Zealand, Mexico and the U.S. grew and developed from IAPH-established partnerships and relationships with the Pacific Region Indigenous Doctors' Congress, Healing Our Spirit Worldwide and the World Indigenous Peoples' Conference on Education.
Additional collaborations include the International Union for Health Promotion and Education, the Canadian Society for International Health and the International Council on Human Rights Policy. Targeted initiatives include the Global STOP TB and a potential opportunity focused on hypertension. Still, increased efforts and support in the area of international Indigenous health and health research are required, given that the health status of these populations remains well below their non-Indigenous counterparts.
Outputs and Outcomes
IAPH has taken the lead in raising awareness about the complex health issues faced by First Nations, Inuit, and Métis (FNIM) peoples of Canada.
Serving as the interface between community and researchers, policy and decision makers, and national and international organizations with vested interests in Aboriginal health, IAPH is now taking its place as a mature leader in the living and changing dynamic entity known as Indigenous health research.
With a mandate to advance a national Aboriginal health research agenda aimed at improved health for FNIM peoples, IAPH has realized the following key outcomes:
- Increased capacity
- Expertise and infrastructure in Aboriginal health research
- Development of community–research relations capable of supporting the self-determination of community and individuals
- Increased relevance of knowledge and knowledge usage for positive impacts on FNIM health and wellbeing
- Ethics-based models for good practice standards in research with Aboriginal communities
Outcomes and outputs in advancing knowledge, building capacity, informing decision making, health and health system/care impacts, and economic and transformative impacts of IAPH are reflected in the following standard graphs designed to show strength in Aboriginal health research in Canada over time.
Advancing knowledge
Gaining strength over time
Figure 1 illustrates the growth of grant funding within the context of the Institute's mandate. The number of grants in the IAPH mandate increased from 15 in fiscal 2000–2001 to the current total of 225 in 2009–2010. Over the same period, the annual dollar value of IAPH mandate grants increased from $1.689 million to $27.289 million. Funding data are based on a keyword search of the CIHR funding database followed by a subjective validation process. Projects may be aligned with the mandates of multiple institutes.
The growth trajectory shown in Figure 1 is consistent with three phases of capacity building. The first phase, 2003–2004, was based on recruitment within the existing academic research community to Aboriginal health research themes. The second phase of growth reflects the development and training of new investigators in research. This is largely attributable to the Aboriginal Capacity and Developmental Research Environments (ACADRE)-Network Environments for Aboriginal Health Research (NEAHR) associated investigative teams and researchers. The third phase represents a combination of ongoing training program efforts, with graduate student trainees moving into academic and research positions, and the recruitment of community research partners into multidisciplinary research theme projects. This process is ongoing and represents a major component of the way forward within IAPH.
Figure 1: CIHR expenditures in IAPH mandate-relevant research
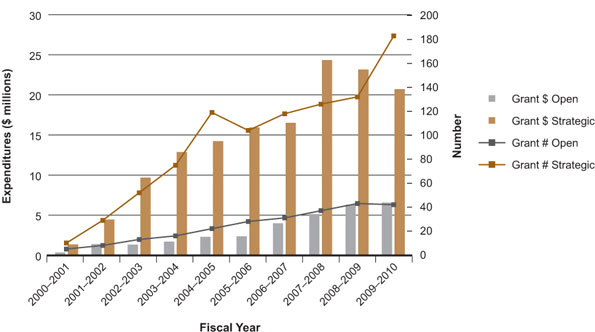
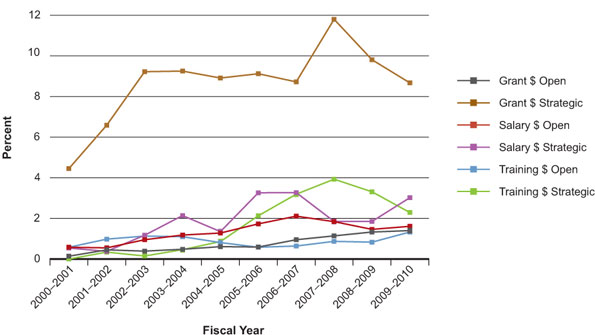
Figure 2 reflects the proportion of funding within the mandate area of IAPH across all grants and awards, both strategic and open. Noteworthy is that the changes show the proportion of CIHR funds in IAPH-related research continues to grow. In 2000–2001, $0.35 million and $1.35 million, respectively, of the total CIHR $247.3 million and $30.3 million were invested in open and strategic grants related to IAPH mandate areas. By 2009–2010, these investments in open and strategic grants had increased to $6.56 million and $20.72 million, respectively, of the total CIHR $468.5 million and $239 million.
As shown in Figure 2, the proportion of CIHR funding in the IAPH mandate area has increased for all grants and awards, a clear indication that a growing proportion of funded health research pertains to Aboriginal peoples or is in line with the CIHR mandate.Footnote 1 From 2000 to 2007 the proportion of funding nearly tripled for strategic grants and quadrupled for training awards. The extra strategic funding through 2007–2009 reflects term funding for northern Aboriginal-focused research within the International Polar Year envelope.
Figure 2: CIHR funding for Aboriginal health research – percentage of total CIHR expenditures related to IAPH mandate areas over time
Bibliometric analysis reveals Canada is in the top three countries producing publications related to Aboriginal health and health research topics. Canada also ranks fourth for average relative citations, higher than some of the countries who rank higher for specialization index (Figure 3 and Table 1).
Figure 3: Specialization index and average of relative citations for top 10 countries publishing in Aboriginal health, 2000–2008
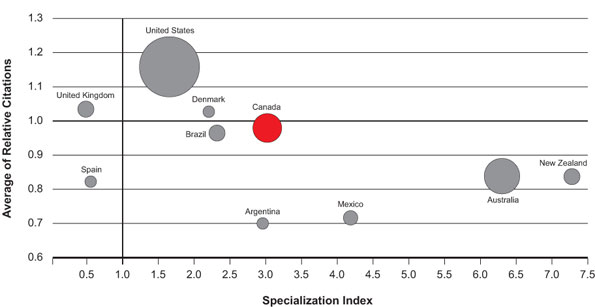
Table 1: Number of publications, average of relative citations and specialization index across top 10 countries in Aboriginal health, 2000–2008
| Country | Number of Publications (2000–2008) | Average of Relative Citations (2000–2008) | Specialization Index (2000–2008) |
|---|---|---|---|
| World | 4,425 | 1.000 | 1.000 |
| United States | 2,311 | 1.165 | 1.640 |
| Australia | 810 | 0.831 | 6.302 |
| Canada | 600 | 0.984 | 3.007 |
| Brazil | 191 | 0.965 | 2.303 |
| New Zealand | 181 | 0.841 | 7.280 |
| United Kingdom | 175 | 1.040 | 0.466 |
| Mexico | 135 | 0.719 | 4.179 |
| Denmark | 94 | 1.033 | 2.187 |
| Spain | 77 | 0.818 | 0.533 |
| Argentina | 74 | 0.702 | 2.947 |
Further exploration of the bibliometrics data identified several authors as NEAHR-associated principal investigators. The most-cited publications relate to clinical studies of chronic disease such as diabetes. This may be in part reflective of the fact that biomedical and clinical research tend to be cited more than research on social or ethical aspects of health or the fact that there are fewer such papers included in the databases used for the bibliometrics work.
Building Indigenous health research capacity – A reflection of increased expertise and infrastructure
NEAHR documents show that several community-based projects have capitalized on their relationships with researchers and funding from the NEAHR (Table 2) to develop successful funding proposals for other granting agencies. For example, NEAHR-funded diabetes seed projects went on to receive $272,000 in funding from two key national funding bodies. Another example is a NEAHR collaboration between community and academic researchers that led to a $100,000 grant for a project on parents with Fetal Alcohol Spectrum Disorder.
Table 2: Number of community grants awarded by the nine NEAHRs from 2007–2010
| A | B | C | D | E | F | G | H | I | |
|---|---|---|---|---|---|---|---|---|---|
| 2010 | 2 | 4 | 2 | 3 | 3 | 2 | |||
| 2009 | 3 | 2 | 4 | 2 | 4 | 1 | 3 | ||
| 2008 | 8 | 1 | 2 | 3 | 1 | 3 | 10 | ||
| 2007 | 6 | 3 | 3 | 4 | 2 | 8 | 3 | ||
| Total | 16 | 11 | 9 | 4 | 4 | 10 | 16 | 7 | 15 |
Key outcomes of capacity building were drawn from a NEAHR impact evaluationFootnote 3 that investigated the period from 2007–2010. Of students surveyed, 94% reported they had received some form of training or guidance in research ethics specific to Aboriginal populations.Footnote 3 Further, approximately 50% of the students now have academic appointments as faculty members or in research positions. Positions held by IAPH-supported students include: territorial chief medical officer, provincial director of Aboriginal health, associate director of the IAPH, and director of National Centre for Collaborative Health.Footnote 3 Impacts of student training by the NEAHRs are exemplified by the following:
"I never could have achieved the quality of research I did for my PhD study without the support and guidance of ACADRE/NEAHR. The support also allowed me the opportunity to share my research with a wide variety of audiences".Footnote 3
Through its NEAHR program, IAPH has enhanced institutional capacity for understanding community ethical considerations. Further, IAPH has and will continue to support communities establishing their own ethics policies and review boards. All nine NEAHR centres report following community ethics in their research. Two regions specifically noted the presence of community-based ethics review boards in their provinces or regions.Footnote 3
"One of the strengths of our network is that we are independent of government authorities and service providers. For example, we were contacted by an Aboriginal organization regarding a serious breach of research ethics taking place in their member communities. We intervened with the government agency to rectify the situation and to ensure that it would not be repeated in other government-sponsored research".Footnote 3
Specialized training programs are another NEAHR outcome. An example is the Clinician Research Mentorship. This program matches Aboriginal medical students or family practice interns with medical doctors engaged in clinical studies and trials. The program is reported to significantly increase student uptake and understanding of the medical health research rocess. The program has received word that there is interest in applying these methods to dentistry.Footnote 3,Footnote 14
Each year IAPH hosts a National Gathering of Graduate Students interested in health research with Aboriginal peoples. The driving objectives of the IAPH National Student Gathering are twofold: the gathering provides graduate students with a forum to identify pressing issues related to their academic development, such as funding, support, isolation and collegiality; and graduate students have the opportunity to network. This shapes the rapidly emerging discipline of Aboriginal health by increasing engagement of student trainees.Footnote 14
A steady increase in attendees, from 39 at the inaugural meeting in 2001 to 85 in 2010, demonstrates increased awareness of IAPH, increases in the mentoring of Aboriginal health researchers and development of research and researcher capacity.Footnote 3,Footnote 14 Students from across disciplines as diverse as economic and environmental sciences demonstrate the increased potential for multidisciplinarity within Aboriginal health research. Several ACADRE-NEAHR student trainees are now considered or emerging as experts in their respective fields.
Informing decision making through knowledge translation
The Institute's NEAHR program, through student mentorship and training, is an important vehicle for knowledge generation in the field of Aboriginal health. For example, NEAHR students reported that a condition of their funding agreement was to develop and implement a knowledge translation (KT) strategy as part of their research protocol.Footnote 3 One student trainee stated, "It is a requirement for my funding from the NEAHR that I have a good KT strategy in place for my own research. This requirement forced me to focus on how this would be accomplished".Footnote 9
A full-time position is dedicated to KT activities at one NEAHR centre. Responsibilities of this position include developing and implementing a comprehensive KT and communications strategy and developing policy for information collection and reporting.
In addition to traditional academic-based approaches to KT such as conference presentations and publications, some NEAHR centres also indicated more coordinated and innovative approaches. Examples include an online health resource centre and information clearing house, the first textbook on mental health for Canadian Aboriginal people and an article entitled Trends in the Study of Aboriginal Health Risks in Canada.Footnote 15
Transforming research knowledge translation and exchange
Integrated KT is a difficult but worthy target. Incorporating knowledge users and decision makers into the planning and design of research projects at the outset shortens the trajectory to effective utilization of the knowledge generated. Integrated KT is implicit in the 2008 CIHR Guidelines for Health Research Involving Aboriginal People.Footnote 2 Knowledge users include the community.
Numerous examples of good practice are ready for scaling up. One example is the respiratory health brought to 68 Inuit children in four Nunavut villages through the work of Dr. Tom Kovesi, a pediatric respirologist, and colleagues from the Canada Mortgage and Housing Corporation.Footnote 16 Another is a study by Colleen Anne Dell and colleagues. They describe their experiences helping addicted First Nations youth at an Ontario solvent-abuse treatment centre.Footnote 17 They draw on a residential school treatment modality grounded in a culture-based model of resiliency. The study is an exercise in knowledge translation.
Research supported by IAPH impacts on health care and health systems. Access projects that introduce community health representatives to urban settings and hospital environments can ease transition impacts between remote or rural Aboriginal communities and tertiary-care centres. Cultural competency and safety training is a component of health professional training throughout Canada but the effects of such training for Aboriginal patients and their families is relatively unexplored. IAPH supports projects that study the impacts of cultural competency training on patient health, including models of training, geographic location of patients and families and differences among Aboriginal groups.
Improving models of good practice and health impacts
All responding NEAHR centres reported that their research was guided by ethical principles as provided in the CIHR guidelines and the new Tri-Council Policy Statement (3). A NEAHR centre reported, "Our centre held a workshop on ethics in research involving Aboriginal peoples. A DVD of the workshop was created as a KT tool. The DVD is currently used in two courses at the University of Victoria and Dalhousie University. The Assembly of Manitoba Chiefs is also using the DVD as a training tool for their staff".Footnote 3
The Institute supports new models of health service delivery such as bringing traditional healers and traditional healing practices into the mainstream and increasing the scope of practice for community health representatives, midwives and other health practitioners. These models must be tested to determine ways to bring modes of treatment and teams of professionals together.
Multidisciplinarity is increasingly important in health and health care systems. It calls for going beyond the conventional biomedical groupings. Health becomes a construct that includes education, economic factors and social networks. Factors related to colonization, such as a breakdown of identity, displacement and disconnection from traditional lands, are viewed as determinants of Aboriginal health.Footnote 18 The relevance of these factors to Aboriginal peoples' health speaks to the need for multidisciplinarity in Aboriginal health research and for experts to engage in related research. Increased community engagement and participation are essential to achieving community and individual wellness.
The Institute has acknowledged these concerns. Funding opportunities such as Aboriginal Health Interventions, launched in 2008, have made multidisciplinary teams a criterion. Principal investigators and theme groups of NEAHR also reflect a high level of multidisciplinarity in their make-up. NEAHR research projects and student initiatives have demonstrated a move by centres toward multidisciplinarity in working with FNIM peoples to improve health delivery systems and models. Examples from the Alberta NEAHR include the Merging Boundaries Conference, designed to bring Aboriginal education and health practitioners together, and the Parallel Pathways New Investigator Grant, which focuses on opportunities for graduate students to learn from traditional healers.
Economic impacts of internal and external partnership investments
The Institute is positioned to improve health and health care systems through partnered investments. Investments include a three-year (2009–2012) financial commitment to a project for understanding the special needs of Aboriginal children with disabilities (Jordan's Principle), an investment by the Province of Ontario in Aboriginal women's health and, most notably, the Aboriginal Health Interventions Research priority announcement launched in 2009.
IAPH anticipates it will contribute to CIHR's goal of decreasing health inequities in Aboriginal peoples and other vulnerable populations by committing at least $1 million a year. Partners will add another $1.5 million. Included are CIHR Knowledge Translation and Ethics programs, First Nations and Inuit Health, Indian and Northern Affairs Canada and Canada's Research Based Pharmaceutical Companies. The first request for applications brought an unprecedented 28. Early indications of success for this priority announcement have led to a second launch planned for December 2009.
Advancing knowledge in Aboriginal health and health research
Several key activities of IAPH advance knowledge in Aboriginal health and health research. For example, a large percentage of IAPH strategic funds is currently used to support the NEAHR program. NEAHR centres must use 40% of allocated funds for student trainees. IAPH also advances knowledge by increasing the Institute's communications and media profile.
In its early years, IAPH maintained a low media profile to concentrate on capacity building. In 2006, CIHR's public affairs department initiated Expert Alerts, profiles of prominent researchers sent to mainstream media outlets. Fifteen researchers profiled over three years were experts in IAPH research areas. In 2009, IAPH placed greater emphasis on reaching Aboriginal media and facilitating direct media interviews, in particular to support knowledge translation and increase communication between researchers and FNIM communities.
Transformative effects of the Institute
Transformation and its effects in relation to Aboriginal peoples is considered a vital aspect of survival. The statement, "transformation is to be anticipated within every living thing participating in the research project" (Weber-Pillwax),Footnote 19 speaks to the significance of change within Indigenous reality.
Achievements of the ACADRE-NEAHR program reflect the significance of change.
Nearly 400 students have been trained in Aboriginal health research, more than 90 community health research projects have been engaged, and academic and community research and researcher capacity has increased as evidenced by the following quote from a 2010 impact evaluation:
"The ACADRE-NEAHR process has been exceptional. Aboriginal communities and organizations are emerging as independent, autonomous and valued partners in the process of engaging in research that is relevant, meaningful and of value to the communities at large. The increasing pool of Aboriginal students and researchers engaged in Aboriginal health research either independently or collaboratively with non-Aboriginal researchers has been a critical motivator for Aboriginal students and communities in viewing research as a future and career."
The transformative effects of IAPH have occurred at multiple levels: individually, in communities, academic institutions, nationally and even internationally through development of the CIHR guidelines.Footnote 2 Developed through extensive regional and national consultations involving the IAPH-NEAHR network, these guidelines aimed to assist researchers and institutions in carrying out ethical and culturally competent research involving Aboriginal people. They became a critical resource in developing the Tri-Council Policy Statement, thereby impacting research carried out with Indigenous Peoples in Canada and abroad.
IAPH fosters a holistic approach to health and health research and has been a key factor in the improving relations between health researchers and Aboriginal communities. A relationship of distrust and negativity has changed to one that has potential to positively influence health and wellness among First Nations, Inuit and Métis communities. As examples of this metamorphosis, communities have engaged respectfully in CIHR-supported research into hereditary disease and predispositions to disease. In both cases, trust has enabled researchers to collect medical information and blood samples.
This represents a complete turnaround from the prevailing sentiment following an incident in 2000 when the Nuu-chah-nulth First Nation, possessing a high prevalence of arthritis-like conditions, agreed to give researchers medical information and blood samples from the community to discover genetic markers of the condition. Samples were subsequently used for different purposes – action unethical even by the standards of the time. Nevertheless, after securing remaining blood samples, the Nuu-chah-nulth Chief continued to support research into the original research question.
Going Forward
The primary objective of the Institute's nine Network Environments for Aboriginal Health Research Centres, and the Aboriginal Health Research Network Secretariat (the coordinating body) is to develop a supportive, advanced research environment in Aboriginal health across Canada.
Transitions within the Institute include the 2009 appointment of Dr. Malcolm King as Scientific Director and development of an evolving set of priorities (2006–2011). IAPH continues to stay dedicated and true to the original intent of its vision and core values. Reflective of the changing needs and priorities of First Nations, Inuit and Métis (FNIM) peoples and in alignment with CIHR's priorities, IAPH is developing its 2011–2016 strategic plan. In the interim, IAPH has re-identified Priority 2, Ensure inclusion and recognition of Aboriginal values and cultures in health research, as a value statement. Priority 4, Resolve critical Aboriginal health issues, is now seen as a vision statement for the future.Footnote 20
In 2009–2010, IAPH carried out a national dialogue with FNIM communities called the Aboriginal Health Research Four Directions Summits Process. The process engaged more than 150 FNIM peoples across more than 10 disciplines, including medicine, nursing, education, addictions treatment and health service delivery. Outcomes continue to transform the Institute as research priorities and areas of critical need are identified. These include: the high incidence of chronic disease; access to Indigenous foods, medicines and healing practices; the health impacts of service gaps; and a lack of community research capacity. Northern and remote areas in particular report a lack of research capacity.
By undertaking such an unprecedented national dialogue with FNIM peoples, IAPH acknowledges the importance of an ongoing dialogue.
The dialogue process was supported by ethical practices such as inclusiveness, community and cultural practices and protocol and, as such, created a safe environment. The environment also recognized the importance of community-level practitioners to the improved health and wellness of Aboriginal peoples.
Factors influencing the Institute's advancement
IAPH's 2006–2011 strategic plan aligns well with CIHR priorities, which has a positive impact on IAPH's ability to respond to changing needs and emerging challenges in Aboriginal health and health research. CIHR's resolve to "decrease health inequities of Aboriginal Peoples and other vulnerable populations"Footnote 1 has positioned IAPH to take a leadership role.
1. Invest in world-class research excellence
The Institute has formed a base of outstanding investigators who are emerging as experts in Aboriginal health and health research through training, mentorship and annual gatherings. Recognizing the need for a fair and transparent peer-review process, IAPH helps recruit experts to serve on the CIHR Aboriginal Health Committee. Community-based methodologies and those grounded in Indigenous epistemologies – central pillars of IAPH – cross disciplines and nations to produce innovative proposals. Research that is relevant and responds to the challenges and opportunities and needs of the Canadian health system is vital to improve the health of Aboriginal and all other Canadians.
2. Address health and health system research priorities
The Institute's renewal plans for NEAHR envision a stronger national collaborative effort vested in improving Aboriginal health. By identifying and taking strategic steps, NEAHR will help communities work toward more accessible and sustainable health care for Aboriginal peoples.
3. Accelerate the capture of health and the economic benefits of health research
IAPH's knowledge translation activities are of paramount significance in light of the populations that the Institute serves. The diversity and particular needs of FNIM Canadians require expertise sensitive to cultural understandings of medicine, health and wellness. For research findings to be used, collaborations between researchers and users of research knowledge must include methods that cross academic and community understandings.
4. Achieve organizational excellence, foster ethics and demonstrate impact
IAPH has provided leadership in ethics and research with Aboriginal peoples in Canada, and with other Indigenous populations that cite CIHR guidelines as enveloping principles of good practice in research. Ongoing support and work with CIHR Ethics and the Tri-Council Policy Statement are two important roles of IAPH in ethics of research. As the lead Institute in the development, implementation and evolution of CIHR's ethics guidelinesFootnote 2 IAPH continues to promote discussions of ethical principles in research with Indigenous populations. Such discussions are key to capacity development, mutually beneficial community engagement and knowledge translation of health research with Aboriginal peoples.
Institute of Aboriginal Peoples' Health leadership
As the only organization of its kind across the globe, IAPH furthers CIHR's vision "to position Canada as a world leader in the creation and use of knowledge through health research that benefits Canadians and the global community." The Institute's pursuit of research excellence is enhanced by respect for community research priorities and Indigenous knowledge, values and cultures. The Institute has stepped lightly in its leadership role while academic and community health research and researcher capacity developed. Since his appointment, IAPH Scientific Director Dr. King has assumed a leadership role in the areas of ethics, northern health, international Indigenous partnerships and the amelioration of health inequities for Aboriginal peoples.
The CIHR priority to decrease ongoing inequities in the health status of Aboriginal peoples is both ambitious and challenging.
IAPH has the potential to build upon the ideals and goals of CIHR and is poised to support other institutes in taking decisive and coordinated action designed to increase the health of Aboriginal peoples.
The institutes of CIHR may then act in unison, synthesizing the health research and spurring the coordinated action needed to significantly improve the health of Aboriginal peoples in Canada.
IAPH has maintained the integrity of its founding set of values. Moving forward, it must actively and persistently ask: What connects the activities of Aboriginal health research and the healing we are trying to support and assist? What are the community benefits, the goals of the partnerships, the guidelines and protocols that must be acknowledged and adhered to in planning and carrying out these activities? What drives and motivates the intended outcomes?
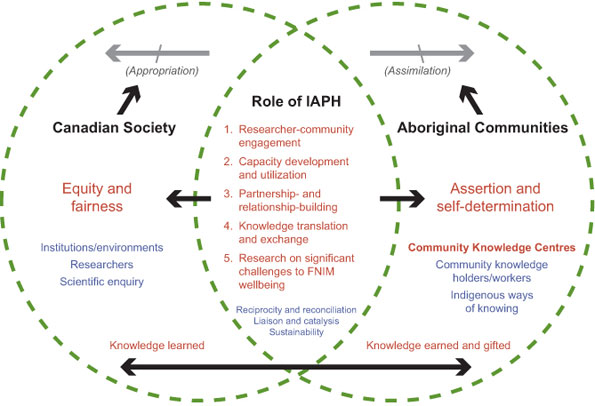
The Summits Process of 2009–2010 led to the development and expression of the following model of two-eyed seeing (Figure 4).
Figure 4: Two-eyed seeing – A model for co-advancement
Vision: Healthy and Well First Nations, Inuit and Métis Peoples
through Community Knowledge and Indigenous Values
Two-eyed seeing means learning to see from one eye with the strengths of Aboriginal peoples' knowledge systems and ways of knowing and from the other eye with the strengths of the mainstream's knowledge systems and ways of knowing – and using these together, for the benefit of all (Albert Marshall, Mi'kmaq Elder, Eskasoni, Nova Scotia). This model shows us the way toward achieving health equity for FNIM peoples. It indicates that community and academic partners have active and equitable roles, and that IAPH is the catalyst for this process of engagement and co-development.
The Institute, as an interface between community and the achievements of modern research, is assisting CIHR in its quest to improve the health of Canada's Aboriginal peoples. Working in harmony with FNIM communities, IAPH continues to make space at the table for Aboriginal health research.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IAPH specific
| ACADRE | Aboriginal Capacity and Developmental Research Environments |
| AIDS | acquired immune deficiency syndrome |
| FNIM | First Nations, Inuit and Métis |
| HIV | human immunodeficiency virus |
| ICCH | International Congress on Circumpolar Health |
| KT | knowledge translation |
| NEAHR | Network Environments for Aboriginal Health Research |
| REB | Research Ethics Boards |
| T2D | Type 2 diabetes |
- Date modified: