2014-15 Departmental Performance Report
Table of Contents
- Minister's Message
- Section I: Organizational Expenditure Overview
- Section II: Analysis of Programs by Strategic Outcome
- Section III: Supplementary Information
- Section IV: Organizational Contact Information
- Appendix: Definitions
- Footnotes
Minister’s Message

I am pleased to present the 2014–15 Departmental Performance Report (DPR) of the Canadian Institutes of Health Research (CIHR).
Research and innovation are the keys to building an effective, efficient, and sustainable health care system. Through CIHR, the Government of Canada is investing in world-class research that will produce the innovations needed to strengthen our health care system and improve the health of Canadians.
In 2015, CIHR celebrated its 15th anniversary. This year also marked the launch of CIHR’s new strategic plan, Health Research Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians. This plan will guide the organization over the next five years, with a focus on supporting research that is innovative, transformative and impactful. The plan affirms CIHR’s commitment to investigator-initiated research, and also sets out four areas of focus for priority-driven research: improving patient outcomes; improving health and wellness for Aboriginal peoples; health promotion and disease prevention; and the treatment of chronic conditions.
During the past year, we witnessed an Ebola epidemic spread throughout the countries of West Africa. CIHR, together with other government partners, played a significant role in the international efforts to respond to the outbreak by supporting a Phase I clinical trial on Canada’s Ebola vaccine (VSV-EBOV).
This year also saw CIHR make significant contributions to the global fight against dementia, with the launch of the Canadian Consortium on Neurodegeneration in Aging. This collaborative research program is focused on finding ways to improve the quality of life and quality of services for those living with neurodegenerative diseases and, hopefully, finding a cure.
CIHR made further progress in the area of mental health with the launch of ACCESS Canada, the inaugural research network under the Strategy for Patient-Oriented Research (SPOR). The network will seek to increase access to mental health services for youth and adolescents. As well, CIHR participated in an Arctic Council symposium which showcased research projects aimed at preventing suicide and building resilience in Northern and Indigenous communities.
The health challenges we face today are complex. They require a coordinated approach that considers patients’ perspectives, brings together the best scientific minds and maximizes our resources. Through CIHR, the Government of Canada is building partnerships and investing in health research that will seek solutions to these challenges for the benefit of Canadians.
The Honourable Jane Philpott, P.C., M.P.
Minister of Health
Section I: Organizational Expenditure Overview
Organizational Profile
- Appropriate Minister: The Honourable Jane Philpott, P.C., M.P.
- Institutional Head: Dr. Alain Beaudet, Deputy Head
- Ministerial Portfolio: Health
- Enabling Instrument: Canadian Institutes of Health Research Act (S.C. 2000, c. 6)Footnote 1
- Year of Incorporation / Commencement: 2000
Organizational Context
Raison d’être
The Canadian Institutes of Health Research (CIHR)Footnote 2 is the Government of Canada’s health research funding agency. The Minister of Health is responsible for this organization. It was created in June 2000 through the Canadian Institutes of Health Research Act (Bill C-13) with a mandate “to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system.”
Responsibilities
CIHR’s mandate seeks to transform health research in Canada by:
- Funding both investigator–initiated research, as well as research on targeted priority areas;
- Building research capacity in under-developed areas and training the next generation of health researchers; and
- Focusing on knowledge translation that facilitates the application of the results of research and their transformation into new policies, practices, procedures, products and services.
CIHR integrates research through a unique interdisciplinary structure made up of 13 “virtual” institutes.Footnote 3 These institutes are not “bricks and mortar” buildings but communities of experts in specific areas. Collectively, the institutes support a broad spectrum of research: biomedical; clinical; health systems and services; and the social, cultural and environmental factors that affect the health of populations. The Institutes form national research networks linking researchers, funders and knowledge users across Canada to work on priority areas.
As Canada's health research funding agency, CIHR makes an essential contribution to the Minister of Health's overall responsibilities by funding the research and knowledge translation needed to inform the evolution of Canadian health policy and regulation, and by taking an advisory role on research and innovation issues. This is achieved through an extensive and growing set of linkages with Health Canada and the Public Health Agency of Canada, providing decision makers with access to high-quality and timely health research outcomes/results.
CIHR also works closely with the Natural Sciences and Engineering Research Council (NSERC)Footnote 4 and the Social Sciences and Humanities Research Council (SSHRC)Footnote 5, the two granting councils of the Industry portfolio, to share information and coordinate efforts, harmonize practices, avoid duplication and foster multidisciplinary research. The three organizations (referred to as “Tri-Agency”) provide a channel for the implementation of common policies, practices and approaches, whenever possible.
CIHR’s Governing Council (GC)Footnote 6 sets the strategic direction of the Agency and is responsible for evaluating its performance. Leadership on research, knowledge translation and funding for research is provided by the Science Council (SC)Footnote 7, while leadership on corporate policy and management is provided by the Executive Management Committee (EMC).Footnote 8
Strategic Outcome and Program Alignment Architecture
In October 2013, the President of the Treasury Board approved a new Program Alignment Architecture (PAA) for CIHR that took effect April 1, 2014 and is reflected in this DPR. The PAA consists of one Strategic Outcome and two Programs that support the Strategic Outcome, as well as internal services. The new PAA structure and descriptions are a complete and accurate inventory of CIHR programs.
The performance information presented in Section II is organized according to this PAA structure as shown below:
- 1. Strategic Outcome: Canada is a world leader in the creation, dissemination and application of health research knowledge
- 1.1 Program: Investigator-Initiated Health Research
- 1.1.1 Sub-Program: Operating Support
- 1.1.2 Sub-Program: Training and Career Support
- 1.2 Program: Priority-Driven Health Research
- 1.2.1 Sub-Program: Institute-Driven Initiatives
- 1.2.2 Sub-Program: Horizontal Health Research Initiatives
- 1.1 Program: Investigator-Initiated Health Research
- Internal Services
Organizational Priorities
In 2014–15, CIHR released its new strategic plan for 2014–15 – 2018–19, Health Research Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians (Roadmap II)Footnote 9. Roadmap II builds on Canada’s reputation as a world leader in health research excellence and embraces new ways of working with partners and stakeholders through a dynamic framework for research investment. It sets three strategic directions that will enable CIHR to provide researchers with the mechanisms to pursue new ideas and mobilize research communities to focus on health priorities that are relevant to Canadians, while maximizing the value and impact of CIHR investments. Due to timing of their release, these three strategic directions will only appear in the 2015–16 Report on Plans and Priorities (RPP) and Departmental Performance Report. In the interim, the organizational priorities outlined in the 2014–15 RPP have been maintained.
Over the past several years, we have worked to modernize our programs, policies and systems to better capitalize on Canada’s health research strengths and to adapt to the evolution within the health research landscape. A bold approach was taken to design a high-quality, flexible and sustainable system capable of identifying and supporting excellence in all areas of health research. CIHR is in the process of transitioning from the existing Open Suite of programs into the new Open Funding Grant programs. The new Open Funding Grant programs are designed to meet the needs of the broad disciplinary mix of researchers within CIHR’s mandate, supported by a new peer review process that addresses many of the current challenges and is intended to reduce the burden felt by applicants and peer reviewers.
Organizational Priorities
| Priority #1 | TypeFootnote i | Programs |
|---|---|---|
|
||
Investigator-Initiated Health Research |
Previously Committed To |
1.1 Investigator-Initiated Health Research |
| Summary of Progress | ||
What progress has been made toward this priority? The reforms of Open ProgramsFootnote 10 aim to contribute to a sustainable Canadian health research enterprise by supporting world-class researchers in the conduct of research and its translation across the full spectrum of health, and to ensure the reliability, consistency, fairness and efficiency of the competition and peer review processes. The design of the new Open Suite of funding mechanisms sets clear objectives for CIHR’s investigator-initiated grants program. This includes integrating CIHR's current suite of Open funding mechanisms into a simpler system that is flexible enough to accommodate today’s changing landscape of health research. As part of the reforms of Open Programs, the Foundation Grant ProgramFootnote 11 was delivered in parallel with a “transitional” Open Operating Grant Program, as well as other ongoing open grant programs on their regular timelines. Competition results will be known in 2015–16. Throughout 2014–15, CIHR continued to validate design elements as a result of pilots run in 2013−14 and by launching four additional pilots in 2014–15. The resultsFootnote 12 and analyses of the fall 2013 Knowledge Synthesis pilotFootnote 13 were published on the CIHR website. Work is also continuing on the establishment of a College of ReviewersFootnote 14 that will ensure the necessary reviewer expertise across the full breadth of CIHR’s mandate. An external advisory group continued to support CIHR in the refinement of the design of the College of Reviewers. In preparation for the first wave of recruitment, reviewer profiles are under development and college members will have the opportunity to validate them as part of their enrollment. CIHR has continued to fund the very best investigator-initiated ideas throughout this transition. A total of 2,862 applications were received for the Open Operating Grant Program.Footnote 15 In 2014–15 the Training and Career Support sub-program funded 397 new master’s trainees, 186 new doctoral trainees and 182 new postdoctoral fellows. |
||
| Priority #2 | Type | Program |
|---|---|---|
Priority-Driven Health Research |
Previously Committed To |
1.2 Priority-Driven Health Research |
| Summary of Progress | ||
What progress has been made toward this priority? CIHR continued to roll out funding opportunities and support the ongoing implementation of the various elements of the Strategy for Patient-Oriented Research (SPOR)Footnote 16 which began in 2013–14. Funding began for two new Support for People and Patient-Oriented Research and Trials (SUPPORT) UnitsFootnote 17 in Quebec and Newfoundland and Labrador, for a total commitment of $24.2M over five years. CIHR support for SPOR now totals $122.5M until 2018–19. In 2014–15, CIHR leveraged $134.2M through its strategic investments and developed new partnership strategies for four existing and emerging Signature Initiatives (large-scale initiatives designed to be transformative and have measurable impact in the near-term) that are driving meaningful engagement with private, public, and charitable sector partners. This includes a new strategic alliance with the National Research Council Industrial Research Assistance Program (NRC-IRAP) and provincial partners to facilitate collaborations between industry, academia and health care providers to bring innovative technology solutions to the health care system. Collectively, these alliances are informing the ongoing development of CIHR’s overall partnership strategy. In 2014–15, CIHR continued to implement its new governance strategy for managing large-scale initiatives to increase the potential for greater impact on patient experiences, health outcomes and a more effective and efficient health care system. |
||
| Priority #3 | Type | Program |
|---|---|---|
Organizational Excellence |
Previously Committed To |
Internal Services |
| Summary of Progress | ||
What progress has been made toward this priority? CIHR has been implementing a wide range of initiatives in response to what was heard from its employees during the 2013−14 Blueprint 2020 consultation sessions. Our progress to date was shared with the Clerk of the Privy Council Office in our progress report dated January 2015. The two key mechanisms currently in place that allow CIHR to support many of the ideas generated through the Blueprint 2020 consultation exercise are the CIHR Human Resources Management Strategy and the Internal Communication Roundtable Action Plan. CIHR is proud of its contribution, both at the agency level and in collaboration with other departments to reach the Blueprint 2020 vision of a “world-class Public Service”. In 2014–15 CIHR began the implementation of an improved performance measurement regime. This toolbox is designed to allow CIHR to better identify and report on the transformational health outcomes of the research funded while creating linkages between each program and allowing CIHR to better report on its achievements. As part of this implementation, CIHR developed and approved 13 performance measurement strategies for most of its Signature and other major initiatives as well as major programs such as the Operating Support Grant Program. CIHR also developed and implemented a new multi-year investment planning process which supports sound financial and risk management practices. This new framework enables governance bodies to focus on CIHR’s proposed health research relevance and impact while using business processes that are clear, nimble, transparent, sustainable and flexible. |
||
Risk Analysis
From its inception, CIHR has endeavored to make a difference in the lives of Canadians by identifying and addressing the health needs of Canadians and investing in health research innovation. This has enabled CIHR to better mobilize, translate and diffuse newly discovered knowledge and research resulting from both the academic and private sectors.
It should be noted that “a revolution is underway in Canada’s health research landscape.” (CIHR, 2014), which is providing opportunities in health research while, at the same time, allowing CIHR to continue to adapt to its ever-changing environment and ensure that investments in health research contribute to the health and well-being of Canadians. Given this new context, as noted earlier, CIHR published a refresh of its five-year strategic plan, Roadmap II, aimed at three broad strategic directions that fully align to CIHR’s PAA. Roadmap II also aligns to the Government of Canada’s newly released update of the Science, Technology and Innovation Strategy – Moving Forward in Science, Technology and Innovation 2014Footnote 18. This strategy outlines continued support for science and innovation including health research innovation. As part of the renewal of its strategic plan, CIHR developed an integrated performance management regime that now informs decision making at CIHR and allows for improved reporting both internally and externally.
The current international austerity climate has resulted in a number of stresses on research funding in general. As a result, CIHR is leveraging private sector and other partners to increase investments in health research. It is anticipated that these collaborations will not only strengthen CIHR’s capacity building efforts but also foster new discoveries to support the innovation pipeline in an effort to make the strongest possible impact on health and health care. This has resulted in the Government of Canada announcing further funding of $13.0M for SPOR, a coalition of federal, provincial and territorial partners dedicated to the integration of research into care, and $2.0M per year to support additional research to better understand and address the health challenges posed by anti-microbial resistant infections.
CIHR strives to maximize value for money and return on its investment through strong stewardship and informed decision making. As a result, risks inform the decision-making process at CIHR and as part of the 2014–15 Report on Plans and Priorities, nine risks were identified that required ongoing monitoring. Three key risks required regular monitoring and reporting by senior executive management; however, with the completion in August 2014 of CIHR’s Governing Council’s “Institutes Model Review” and resulting decisions, this risk rose from moderate to a high-level status, requiring ongoing monitoring by senior executives. The top four risks are outlined below, including the “Institutes Model Review”, along with the associated actions and mitigation strategies undertaken by CIHR.
2014–15 Key Risks
| Risk 1 – Alignment and Priority Setting | Risk Response Strategy | Link to Program Alignment Architecture |
|---|---|---|
There is a risk that CIHR will lack the funds needed to support the ever-changing environment that currently exists in health research and that CIHR’s current budget allocation will negatively impact our ability to strategically invest in priority health areas. |
Alignment and Priority Setting was identified in the 2014–15 Report on Plans and Priorities (RPP) and the 2014–15 Corporate Risk Profile (CRP). CIHR responded to this risk by:
Additionally, the following mitigation strategies which were not included in the 2014–15 RPP were completed:
While much was accomplished to mitigate this risk, Alignment and Priority Setting remains a high risk and will be actively managed by CIHR in 2015–16. |
Priority-Driven Health Research program |
| Risk 2 – Implementation of the Reforms | Risk Response Strategy | Link to Program Alignment Architecture |
|---|---|---|
There is a risk that CIHR will be unable to successfully implement the new internal processes, policies and structures in the timeframe required to support the reforms, and there is a further risk that the implementation of the technical system will not be completed in the timeframe required to fully deliver on the benefits of the reforms. |
Implementation of the Reforms was identified in the 2014–15 RPP and the 2014–15 CRP. CIHR responded to this risk by:
Significant progress has been made through the mitigation strategies related to this risk, and as a result Implementation of the Reforms is no longer a high risk that requires regular and active management by CIHR. |
Investigator-Initiated Health Research Internal Services |
| Risk 3 – Human Resources | Risk Response Strategy | Link to Program Alignment Architecture |
|---|---|---|
There is a risk that CIHR will not have the right skill set to deliver on CIHR’s key priorities in the ever-changing health research environment, coupled with the impact the reforms will have on CIHR’s current skill set. |
Human Resources was identified in the 2014–15 RPP and the 2014–15 CRP. CIHR responded to this risk by:
Additionally, the following mitigation strategies which were not included in the 2014–15 RPP were completed:
Human Resources is now a moderate risk for CIHR as a result of its mitigation strategies and is no longer a high risk for CIHR in 2015–16 but will continue to be monitored. |
Strategic Outcome: Canada is a world leader in the creation, dissemination and application of health research knowledge. Internal Services |
| Risk 4 – Institutes Model Review | Risk Response Strategy | Link to Program Alignment Architecture |
|---|---|---|
There is a risk associated with the Institutes Review that CIHR will be unable to make needed program, policy or other changes to adapt to, or efficiently meet emerging or evolving needs. |
The Institutes Model ReviewFootnote 19 was originally identified as a moderate risk in the 2014–15 CRP and, as such, it was not included in the 2014–15 RPP. As a result of the Institutes Model Review and the significant work required to implement the Governing Council’s recommendations, it was moved to a “high” risk status. CIHR responded to this risk by:
Significant progress has been made related to the Institutes Model Review and the risk no longer appears in CIHR’s Corporate Risk Profile for 2015–16. Of the various directions set by Governing Council, some were completed or are in progress. Components of the Institutes Model Review are now included in both the Change Management and the External Stakeholder Relationship Management risks moving forward. |
Strategic Outcome: Canada is a world leader in the creation, dissemination and application of health research knowledge. Internal Services |
Actual Expenditures
| 2014–15 Main Estimates |
2014–15 Planned Spending |
2014–15 Total Authorities Available for Use |
2014–15 Actual Spending (authorities used) |
Difference (actual minus planned) |
|---|---|---|---|---|
984,951,962 |
988,670,351 |
1,018,035,463 |
1,017,279,383 |
28,609,032 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
406 |
419 |
13 |
| Strategic Outcome, Programs and Internal Services | 2014–15 Main Estimates |
2014–15 Planned Spending |
2015–16 Planned Spending |
2016–17 Planned Spending |
2014–15 Total Authorities Available for Use |
2014–15 Actual Spending (authorities used) |
2013–14 Actual Spending (authorities used) |
2012–13 Actual Spending (authorities used) |
|---|---|---|---|---|---|---|---|---|
Strategic Outcome: Canada is a world leader in the creation, dissemination and application of health research knowledge |
||||||||
Investigator-Initiated Health Research |
729,381,763 |
731,743,352 |
703,091,433 |
709,009,132 |
733,531,514 |
726,255,103 |
717,201,006 |
718,241,256 |
Priority-Driven Health Research |
252,550,887 |
253,695,089 |
294,561,829 |
285,625,753 |
281,195,815 |
287,739,904 |
277,820,532 |
275,634,722 |
Subtotal |
981,932,650 |
985,438,441 |
997,653,262 |
994,634,885 |
1,014,727,329 |
1,013,995,007 |
995,021,538 |
993,875,978 |
Internal Services Subtotal |
3,019,312 |
3,231,910 |
12,330,738 |
12,316,287 |
3,308,134 |
3,284,376 |
2,950,450 |
3,176,764 |
Total |
984,951,962 |
988,670,351 |
1,009,984,000 |
1,006,951,172 |
1,018,035,463 |
1,017,279,383 |
997,971,988 |
997,052,742 |
Spending and FTE Variance Explanations
CIHR received an additional $20.0M for various strategic health research initiatives in Budget 2014. This new funding includes $5.0M for SPOR, $5.0M for the Canadian Consortium on Neurodegeneration in Aging (CCNA),Footnote 20 $5.0M for the Emerging Health Threats Research Fund, including Ebola, and $5.0M over 5 years for the Canadian Research Initiative in Substance Misuse (CRISM).Footnote 21
CIHR’s actual spending for 2014–15 is $1,017.3M, with planned spending going from $1,010.0M in 2015–16 to $999.5 million by 2017–18. The variance in CIHR’s planned spending is anticipated to be temporary and spending is expected to increase as a result of additional funding allocated for Tri-Agency programs and partnership activities.
CIHR collaborates with NSERC and SSHRC in a series of Tri-Agency programs, such as the Networks of Centres of Excellence (NCE),Footnote 22 the Centres of Excellence for Commercialization and Research (CECR),Footnote 23 the Business-Led Networks of Centres of Excellence (BL-NCE),Footnote 24 and the Canada Research Chairs (CRC)Footnote 25 and Canada Excellence Research Chairs (CERC).Footnote 26 Funding allocated to each of the three agencies for these programs can vary between competitions depending on the recipients’ alignment with the research mandate and priorities of each agency. Accordingly, funding allocations are confirmed and included in planned spending once the results of each competition are available. As such, CIHR’s planned spending may increase as a result of successful health-oriented projects within the competitions.
CIHR also collaborates on partnership activities with other federal departments and, as a result, funding may be transferred to CIHR to address a common theme or research priority. As partnership activities are confirmed in the upcoming fiscal years, it is anticipated that CIHR’s planned spending will increase.
Please note that the variance in planned spending for internal services for 2015–16 and 2016–17 reflect the RPP for 2015–16 and not the RPP for 2014–15. The reason is that the resources outlined in the 2014–15 RPP do not reflect CIHR’s revised methodology as per the Treasury Board of Canada Secretariat Guide on Expenditures Internal Services: Recording, Reporting and Attributing, which came into effect on April 1, 2015. The implementation of the revised methodology results in administrative resources previously aligned to CIHR’s programs being reallocated to Internal Services. It should be noted also that work is ongoing and further changes will be provided in the 2015–16 DPR and 2016–17 RPP to ensure that CIHR is fully compliant with the new TBS requirements.
Alignment of Spending With the Whole-of-Government Framework
| Strategic Outcome | Program | Spending Area | Government of Canada Outcome | 2014-15 Actual Spending |
|---|---|---|---|---|
Canada is a world leader in the creation, dissemination and application of health research knowledge |
1.1 Investigator-Initiated Health Research |
Social Affairs |
Healthy Canadians |
726,255,103 |
1.2 Priority-Driven Health Research |
Social Affairs |
Healthy Canadians |
287,739,904 |
| Spending Area | Total Planned Spending | Total Actual Spending |
|---|---|---|
Economic Affairs |
0 |
0 |
Social Affairs |
985,438,441 |
1,013,995,007 |
International Affairs |
0 |
0 |
Government Affairs |
0 |
0 |
Departmental Spending Trend
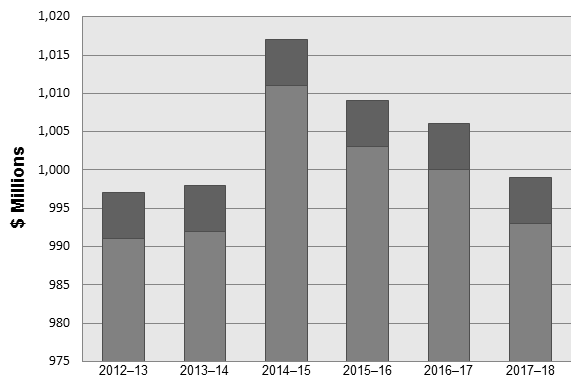
| 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | |
|---|---|---|---|---|---|---|
| Sunset Programs – Anticipated | 0 | 0 | 0 | 0 | 0 | 0 |
| Statutory | 6 | 6 | 6 | 6 | 6 | 6 |
| Voted | 991 | 992 | 1,011 | 1,003 | 1,000 | 993 |
For explanations regarding the variances above, please see the section on Spending and FTE Variance Explanations earlier in this section.
Expenditures by Vote
For information on CIHR’s organizational voted and statutory expenditures, consult the Public Accounts of Canada 2015,Footnote 28 which is available on the Public Works and Government Services Canada website.Footnote 29
Section II: Analysis of Programs by Strategic Outcome
Strategic Outcome: A world-class health research enterprise that creates, disseminates and applies new knowledge across all areas of health research
Distribution of 2014–15 Actual Spending by Program
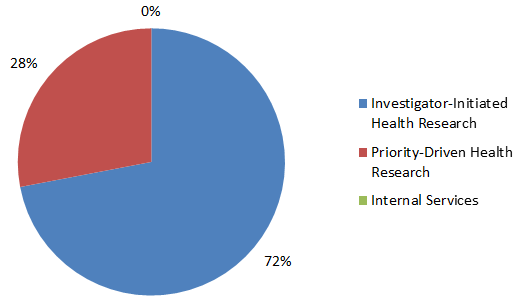
| Investigator-Initiated Health Research | Priority-Driven Health Research | Internal Services |
|---|---|---|
| 72% | 28% | 0% |
Distribution of 2014–15 Actual FTEs by Program
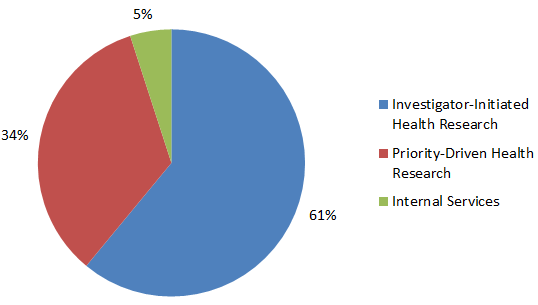
| Investigator-Initiated Health Research | Priority-Driven Health Research | Internal Services |
|---|---|---|
| 61% | 34% | 5% |
CIHR is the Government of Canada's health research investment agency. Overall, in 2014–15, CIHR supported more than 13,000 researchers and trainees in the fulfillment of its mission: to create new scientific knowledge and to enable its translation into improved health, more effective health services and products, and a strengthened Canadian health care system.
CIHR is guided by a peer review system that supports the selection of the most innovative and cutting-edge proposals for research and/or knowledge translation, while continuing to be fair, well-managed and transparent. In 2014–15, approximately 2,790 peer reviewers provided their time, without remuneration, and served on over 188 peer review committees to help review over 11,000 applications.
Health Research in Action
There are more than 13 million shift workers in North America alone. Recent research suggests that shift workers are at increased risk of breast and colon cancer, heart disease, depression and anxiety disorders, and obesity. A potential major factor responsible for these negative health effects is exposure to light at night. Dr. Robert Casper received a grant for a total of $0.5M through the Open Operating Grant Program to study the prevention of circadian rhythm disruption by nocturnal light exposure. Nocturnal light exposure has been shown to disrupt the circadian secretion patterns of hormones such as melatonin and cortisol, as well as clock gene expression, both functions having a 24-hour cycle. There is also evidence that circadian rhythm disruption by light may affect sleep efficiency and shift work performance, especially alertness at the end of a night shift. The need for an economical, physiologically effective method to prevent the adverse effects of nocturnal lighting on circadian rhythm disruption is crucial. Dr. Casper’s team has developed lenses that filter low wavelength light and have shown in animal and clinical studies that it is possible to prevent circadian rhythm disruption by light at night. In the present study, they showed that filtering short wavelengths by having subjects wear optical filter glasses during their night shift, resulted in improved sleep duration and efficiency, measured objectively by polysomographic (EEG) studies, on the first night off after their rotating shift. In addition, the team found that the subjects had improved alertness and improved performance, especially at the end of the night shift when most errors and accidents occur.
For more examples of Health Research in Action, please visit CIHR’s website.
Program 1.1: Investigator-Initiated Health Research
Description
To develop and support a well-trained base of world-class health researchers and trainees conducting research across all aspects of health, including biomedical research, clinical research, research respecting health systems, health services, the health of populations, societal and cultural dimensions of health and environmental influences on health, and other research as required. The goal of this program is to advance health knowledge and to apply this knowledge in order to improve health systems and/or health outcomes. Grants and awards are disbursed to fund research or to provide career or training support. The specific area of research is identified by the researcher.
| 2014–15 Main Estimates |
2014–15 Planned Spending |
2014–15 Total Authorities Available for Use |
2014–15 Actual Spending (authorities used) |
2014–15 Difference (actual minus planned) |
|---|---|---|---|---|
729,381,763 |
731,743,352 |
733,510,617 |
726,255,103 |
-5,488,249 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
251 |
254 |
3 |
| Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
Canada has an internationally competitive health research community |
Canada's health research specialization index ranking versus international levels (G7 nations) |
3rd among G7 |
Canada was ranked 2nd in the health research specialization index when compared to other G7 nations. This is slightly higher than the ranking from previous years. |
CIHR-funded research has improved the health of Canadians |
Percent of CIHR grants reporting contribution to improved health for Canadians |
30% |
CIHR met the 2014–15 target by supporting grants of which 34% reported having contributed to improved health for Canadians. This is consistent with the 2013−14 results. |
Canadian health researchers advance health research knowledge |
Canada's ranking among G7 in health research publications per million dollars of gross domestic expenditure on research and development (GERD) |
2nd among G7 |
Canada was ranked 3rd in health research publications per million dollars of gross domestic expenditure on research and development (GERD) compared to other G7 nations. This is slightly lower than the target but consistent with data from previous years. |
Performance Analysis and Lessons Learned
The variance between planned and actual spending of approximately $5.5M is primarily due to the sun-setting of the Small Health Organization Partnership and Youth Engagement programs ($2.0M) and the internal reallocation of program funds to the Institute-Driven Initiatives sub- program to fund high-quality research in priority health areas. The variance between planned and actual FTEs is due to the creation and staffing of temporary positions related to the Open Programs reforms transition plan.
As part of the new Open Suite of programs, CIHR received 1,366 eligible Stage 1 applications to the first Foundation Grant Program “live pilot” competition. CIHR has invited 467 applicants to submit a Stage 2 application. It is anticipated that between 150-210 applications will be funded in this first pilot. A minimum of 15% of the funded grants will be allocated to new/early career investigators. The new Open Funding Grant Programs will continue to be phased-in during the next fiscal year with the launch of the second Foundation Grant Program and the first Project Grant Program “live pilot” competitions in March 2015.
CIHR has emphasized the importance of piloting key design elements as part of the reforms transition plan. Refinements have already been implemented as a result of early pilot results, and include more comprehensive training materials for applicants and reviewers, and technology enhancements to improve usability. CIHR has also developed a new rating scale for peer reviewers and established a virtual chair/moderator role to improve the consistency and efficiency of the peer review process.
Through both CIHR and Tri-Agency program competitions in 2014–15, CIHR invested $58.4M by funding 1,416 new trainees including master’s, doctoral, postdoctoral or (post) health professional degrees in Canada and abroad. A total of 576 new awards were provided, representing a total commitment of $52.1M over the next 5 years, which includes expenditures of $19.9M in 2014–15 to support highly trained individuals. These results indicate that both total numbers and expenditures remained stable in 2014–15.
In total, CIHR surpassed its expected 1,725 new grants and awards by supporting a total of 1,893 researchers through the Investigator-Initiated Health Research Program. This is an increase from the 1,494 new grants and awards supported in 2013−14.
Sub-Program 1.1.1: Operating Support
Description
Provides grant funding to researchers to conduct research in any area related to health aimed at the discovery and application of knowledge. Investigators identify and propose the nature and scope of the research and compete for support by demonstrating the potential impact the research will have with respect to improving health systems and/or health outcomes. Funding is mainly disbursed through the Open Operating Grant Program and can be used to cover the cost of the research project, consultation fees and fees paid to research participants, for instance. Other transfer payment programs disbursing funding include College and Community Innovation, and Research Chairs for Colleges.
| 2014–15 Planned Spending |
2014–15 Actual Spending |
2014–15 Difference (actual minus planned) |
|---|---|---|
552,687,138 |
552,865,912 |
178,774 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
220 |
224 |
4 |
| Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
CIHR funded health research advances health research knowledge |
Percent of CIHR operating support grants reporting creation of new health knowledge |
90% |
CIHR met the 2014–15 target by supporting grants of which 94% reported having created new knowledge. This is consistent with the 2013−14 results. |
CIHR funded health research results in knowledge translation |
Percent of CIHR operating support grants reporting translation of knowledge |
60% |
CIHR met the 2014–15 target by supporting grants of which 60% reported having translated knowledge. This is consistent with the 2013−14 results. |
CIHR-funded health research findings contribute to health care system improvements |
Percent of CIHR operating support grants reporting contributions to strengthening the Canadian health care system |
25% |
CIHR met the 2014–15 target by supporting grants of which 30% reported having contributed to strengthening the Canadian health care system. This is consistent with the 2013–14 results. |
Performance Analysis and Lessons Learned
For information on the spending and human resources variances, please see the section on Investigator-Initiated Health Research.
In 2014–15, CIHR, through the Open Operating Grant Program (OOGP) competition, funded 802 new grants for a total commitment of $492.9M, thus meeting the goal for the year; these results are consistent with previous years, with a total of 801 new grants supported in 2013–14. These new grants comprise multi-year investments that will aim to make health services and products more effective, and strengthen the Canadian health care system.
As committed to in the RPP, CIHR continued to support 80 knowledge translation grants for a total of $6.9M and 70 commercialization grants worth $9.4M in 2014–15. Announcements were made to the community that the final launch of these programs would take place in 2015–16 before these programs are fully consolidated into CIHR’s new Open Suite of programs.
The Tri-Agency College and Community Innovation program (CCI)Footnote 30 is intended to provide companies that operate from a Canadian base access to the unique knowledge, expertise and capabilities available at Canadian colleges and to train students in essential technical skills required by companies. In 2014–15, two applications related to health research were approved for funding under this Tri-Agency program.
As CIHR prepares to transition away from the long-standing, traditional investigator-initiated programs to a new suite of Foundation and Project grants together with new peer review processes, we have learned the value of systematic, ongoing dialogue with stakeholders across Canada. Over the last few years, CIHR management has reached out through over 230 engagement visits to researchers and administrators at institutions across Canada. This involved repeat visits to institutions through the different phases of the change process, and the creation of standing advisory committees comprising various stakeholders. This dialogue is leading both CIHR and the health research community to successfully navigate large scale change.
Sub-Program 1.1.2: Training and Career Support
Description
Provides award funding to promising researchers and trainees to support training (master's, PhD, postdoctoral fellow) or career advancement (chairs, salary awards) in order to continue to build and maintain Canada's health research capacity across all aspects of health research. Funds are disbursed through the following transfer payment programs: the Fredrick Banting and Charles Best Canada Graduate Scholarships; the Vanier Canada Graduate Scholarships; the Banting Postdoctoral Fellowships; the Canada Research Chairs and the Canada Excellence Research Chairs, and can be used to cover such expenses as research equipment, materials and research supplies or travel to scientific meetings.
| 2014–15 Planned Spending |
2014–15 Actual Spending |
2014–15 Difference (actual minus planned) |
|---|---|---|
179,056,214 |
173,389,191 |
-5,667,023 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
31 |
30 |
-1 |
| Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
Investing in health researchers builds Canada's health research capacity |
Canada's ranking among G7 nations for health researchers per thousand workforce |
3rd among G7 |
In 2011, Canada was ranked 2nd among the G7 (data is only available every 5 years) thus exceeding the target. |
Health researchers receive training and career support through CIHR funding |
Total number of researchers supported through salary and training awards by CIHR |
2,100 researchers supported through new and ongoing awards |
CIHR supported 2,457 researchers through salary and training awards. A recent change in the administration of the CGS Master’s program has resulted in an increase in the total number of awards funded on a fiscal year basis. As a result, CIHR met the 2014–15 target and the methodology for future targets will be revised to reflect this change. |
Performance Analysis and Lessons Learned
For information on the spending and human resources variances, please see the section on Investigator-Initiated Health Research.
In 2014–15, CIHR offered training and salary support through various CIHR and Tri-agency programs. Training and salary awards provided support and special recognition to 158 new CIHR fellowships and 7 doctoral foreign study awards. CIHR also funded 56 new three-year Vanier Canada Graduate Scholarships,Footnote 31 representing a CIHR investment of $8.4M over 3 years, as well as 23 new two-year Banting Postdoctoral Fellowship (PDF)Footnote 32 awards representing a CIHR investment of $3.22M over 2 years. These results are consistent with the numbers from 2013−14.
The Canada Research Chairs program (CRC) stands at the centre of a national strategy to make Canada one of the world’s top countries in research and development. Approximately $265.0M per year is invested to attract and retain some of the world’s most accomplished and promising minds. Tier 1 CRCs have a value of $0.2M per year, and Tier 2 CRCs have a value of $0.1M per year. In 2014–15, CIHR funded 98 new awards through the CRC program – 53 new Tier 1 Chairs (for $ 10.6M) and 45 new Tier 2 Chairs (for $ 4.5M). These results show a slight increase from the previous year, which reported 90 new awards for $8.5M.
Through the Canada Excellence Research Chair (CERC) program, CIHR contributed to building and maintaining world-class research by supporting Canadian universities in their efforts to build on Canada’s growing reputation as a global leader in research and innovation. In 2014–15, CIHR awarded a total of $8.9M through the CERC Tri-agency program for 7 Chairs. This is consistent with the results from 2013−14.
Work continues over a three-year time frame to harmonize the design of the CGS doctoral programs. The long lead time is required in order to permit onboarding of the programs on a single electronic platform that will reduce the administrative burden for the application process in the future.
In total, 962 new training and salary awards were funded through the Training and Career Support sub-program. This is an increase from the results in 2013−14, which show a total of 696 new training and salary awards.
In 2014−15, the Vanier CGS program underwent its first evaluation, which was led by CIHR in partnership with NSERC and SSHRC. The evaluation identified some challenges including the program’s ability to attract and recruit students from outside of Canada. The evaluation recommended that a portion of nomination allocations be reserved for foreign students moving forward. Changes to the three-year cycle allocation and application processes were also recommended to enable the Vanier CGS awards program to better meet its objective of attracting and recruiting world-class doctoral students to Canadian universities. CIHR has changed the allocation of the program to an annual quota, and clearer definitions and guidelines were developed with the dissemination to be included in the June 2015 launch. CIHR continues to work on improvements related to the timing of the program and the recruitment of foreign students to the program.
The CERC program also underwent an evaluation. The evaluation identified some challenges including the program’s need to develop clearer definitions and expectations regarding branding, sustainability, as well as collaborations, partnerships and relationships with users of research (non-academic sectors). These recommendations will be addressed in 2015–16.
Program 1.2: Priority-Driven Health Research
Description
CIHR provides funding to researchers for emergent and targeted research that responds to the changing health needs and priorities of Canadians across all aspects of health, including biomedical research, clinical research, research respecting health systems, health services, the health of populations, societal and cultural dimensions of health and environmental influences on health, and other research as required. The goal of this program is to advance health knowledge and its application, in specific areas of research identified by CIHR in consultation with other government departments, partners and stakeholders, in order to improve health systems and/or improve health outcomes in these priority areas. Grants are disbursed to fund research or to provide career or training support.
| 2014–15 Main Estimates |
2014–15 Planned Spending |
2014–15 Total Authorities Available for Use |
2014–15 Actual Spending (authorities used) |
2014–15 Difference (actual minus planned) |
|---|---|---|---|---|
252,550,887 |
253,695,089 |
281,186,545 |
287,739,904 |
34,044,815 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
132 |
142 |
10 |
| Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
CIHR-funded research contributes to a stronger health care system |
Percent of CIHR grants reporting contributions to strengthening the Canadian health care system |
Baseline Year |
35% of CIHR grants reported contributions to strengthening the Canadian health care system. Although this was a baseline year, CIHR used the data available to determine that the 2013−14 result was 34%. These results are consistent; however, significant changes could occur moving forward as data availability increases each year as more and more programs begin receiving results through CIHR’s Research Reporting System. |
CIHR-funded research advances knowledge in emergent and specific health priorities |
Percent of priority-driven grants reporting creation of new health knowledge |
Baseline Year |
88% of priority-driven grants reported creating new health knowledge. Although this was a baseline year, CIHR used the data available to determine that the 2013−14 result was 90%. These results are consistent; however, significant changes could occur moving forward as data availability increases each year as more and more programs begin receiving results through CIHR’s Research Reporting System. |
CIHR-funded research in emergent and specific health priorities results in knowledge translation |
Percent of priority-driven grants reporting knowledge translation |
Baseline Year |
78% of priority-driven grants reported having translated knowledge. Although this was a baseline year, CIHR used the data available to determine that the 2013−14 result was 70%. The slight increase in results is due to increased data availability as more and more programs begin receiving results through CIHR’s Research Reporting System. |
Performance Analysis and Lessons Learned
The variance between planned and actual spending of approximately $34.0M is due to new funds received in Budget 2014 of $15.0M for various strategic health research initiatives and funds received for the CECR and the Business-led NCE through Supplementary Estimates. New funding includes $5.0M for the Strategy for Patient-Oriented Research (SPOR), $5.0M for the Canadian Consortium on Neurodegeneration in Aging (CCNA) and $5.0M for the Emerging Health Threats Research Fund, including Ebola. The variance between planned and actual FTEs is due to the creation and staffing of positions related to CIHR’s stakeholder engagement and business development priority, as well as internal support related to increased funding in the Priority-Driven Health Research program.
In Budget 2014Footnote 33, the Government of Canada committed a further $5.0M a year on an ongoing basis for the SPOR. As one of the key components for SPOR, funding for the first two SPOR networks was initiated in 2014–15. The first focuses on Adolescent and Youth Mental Health and an agreement was signed with ACCESS Canada. The second network, on Primary and Integrated Health Care Innovations, rolled out using a phased approach; funding for phase II is set to begin in September 2015.
As part of another component of SPOR, implementation plans and first-year annual reports were received for the SUPPORT Units in Alberta, Manitoba, Ontario and the Maritimes. Grant agreements were signed and funding was provided for SUPPORT Units in Quebec ($15.9M) and Newfoundland and Labrador ($9.5M). In 2014–15, CIHR provided development funding of $0.8M for a SUPPORT Unit in the North West Territories. CIHR continued to support the development of SUPPORT Units in British Columbia, Saskatchewan, the Yukon and Nunavut. These shared investments in patient-oriented research will provide necessary and often highly specialized expertise through multidisciplinary centres and other experts who are essential to the patient-oriented research enterprise.
The Canadian Clinical Trials Coordinating Centre (CCTCC)Footnote 34 was created to strengthen the environment for clinical trials in Canada, including the streamlining of processes for companies and researchers, with an aim to regaining Canada’s competitive advantage for hosting clinical trials. This will be achieved by implementing the recommendations from the 2011 Clinical Trials Summit Action Plan. It is a collaborative effort of CIHR, Canada’s Research-Based Pharmaceutical Companies (Rx&D), and HealthCareCAN (formerly ACAHO). In its first year of funding, the CCTCC has established a headquarters, developed a website and other communications materials, and put in place an Advisory Group and other working groups.
In September 2014, the Government of Canada launched the Canadian Component of the CIHR Dementia Research Strategy,Footnote 35 the Canadian Consortium on Neurodegeneration in Aging (CCNA). The Government of Canada, through CIHR, and many partners (provincial, private and not-for-profit) have collectively invested a total of $32.5M over five years towards the CCNA. As a direct result of this funding, the CCNA and the Medical Research Council’s Dementias Platform UK signed a new agreement in March 2015 to more easily share data and research expertise in an effort to better understand, treat and prevent dementia.
CIHR, as part of the Pathways to Health Equity for Aboriginal Peoples SignatureFootnote 36 Initiative, also funded three National Aboriginal Organizations as Partners for Engagement and Knowledge Exchange (PEKEs) ($3.0M) in 2014–15. Additionally, nine Implementation Research Teams received development grants totalling $0.9M. The second phase of the program (to support enhancement and adaptation grants) was also launched this fiscal year.
Finally, as committed to in the RPP, through extensive consultation, the CIHR HIV/AIDS Research InitiativeFootnote 37 developed its Strategic Plan for 2015–20. The Initiative worked in collaboration with its partners in the Federal Initiative to Address HIV/AIDS in Canada to develop a new Implementation Science Initiative for the Prevention of HIV, Hepatitis C and Sexually Transmitted Infections. The first funding opportunity under the multi-phase initiative will be launched early in 2015–16. Additionally, the partnership with the Bill & Melinda Gates Foundation on HIV vaccine research was fully implemented with new investments of $3.4M over three years to support three new team grants.
Further achievements regarding CIHR’s Institute-Driven initiatives and Horizontal Health Research initiatives can be found in the following sections.
Sub-Program 1.2.1: Institute-Driven Initiatives
Description
Provides targeted grant and award funding to mobilize researchers, health practitioners and decision makers to work together to address priority health challenges. These priority areas are identified by CIHR in consultation with partners and stakeholders. Researchers compete for funding by demonstrating the potential impact the research will have with respect to addressing priority areas. Funds may be used to cover such expenses as stipends and salaries. Funds are disbursed through the institute support grant transfer payment program.
| 2014–15 Planned Spending |
2014–15 Actual Spending |
2014–15 Difference (actual minus planned) |
|---|---|---|
187,697,630 |
209,164,968 |
21,467,338 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
111 |
118 |
7 |
| Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
Partners invest in institute-driven research |
Ratio of leveraged funds for institute-driven initiatives |
$1 : $0.30 |
$1 : $0.38 This result shows a slight increase in the ratio of leveraged funds from 2013−14. The increase is due, in part, to a change in the methodology used to capture partner investments. The methodology for future targets will be revised to reflect this change. |
Stakeholders collaborate on institute-driven research |
Percent of institute-driven grants reporting stakeholder involvement in the research process |
Baseline Year |
94% of institute-driven grants reported stakeholder involvement in the research process. This is an increase from the previous year, which showed a total of 70%. This result is due, in part, to the dramatic increase in the data available for this fiscal year compared to previous years as the Research Reporting System brings more and more programs online and results are received. |
Performance Analysis and Lessons Learned
For more information on the variance between planned and actual spending and human resources, please see the section on the Priority-Driven Health Research program.
In 2014–15, CIHR engaged in key national and international strategic partnerships and consortia in order to advance shared priorities and tackle complex, pressing health research challenges. As part of Budget 2014, CIHR received $5M in ongoing funding for the Emerging Threats Health Research Initiatives, the first two years of which is focused on funding for Ebola vaccine research.
CIHR, as the Canadian representative, has taken a leading role the Joint Programming Initiative on Antimicrobial Resistance (JPIAMR),Footnote 38 supporting the Canadian component of six international teams. Funding began in January 2015 for a period of three years. The research is focused on the identification of new targets for antibiotic development, antibiotic discovery and therapeutics to inhibit the mechanisms of resistance and re-sensitize resistant bacteria to existing compounds. Through those six teams, CIHR has invested $4.0M and an additional $6.5M was provided from the 10 partner countries.
CIHR also participated in a partnership with 10 European member states and New Zealand through the Joint Programme Initiative Healthy Diet for a Healthy Life (JPI HDHL).Footnote 39 Through this partnership, CIHR launched a strategic funding opportunity on Biomarkers for Nutrition and Health in order to foster transnational research collaborations in this area. CIHR was able to leverage its contribution of $0.45M to support one of two funded research teams for a total of $7.0M.
In 2014–15, through ongoing partnerships with the Global Alliance on Chronic Disease,Footnote 40 as part of the SPOR Networks, CIHR also launched a funding opportunity for the development and implementation of up to four pan-Canadian networks that focus on non-communicable chronic diseases. Each network will receive $25.0M – $12.5M from CIHR to be matched with funding from non-federal sources.
Finally, as part of Canada’s chairmanship of the Arctic Council, CIHR, in collaboration with the Public Health Agency of Canada, ran a competition to support a participatory, community-based, evaluation on mental wellness promotion and suicide prevention in circumpolar communities, with a particular focus on Indigenous youth. CIHR invested in two research grants for a total of $0.5M. CIHR also partnered to organize a Symposium in Iqaluit, Nunavut, and a travel award competition was subsequently launched to support Canadian youth participation to this symposium and 21 travel awards were funded.
Sub-Program 1.2.2: Horizontal Health Research Initiatives
Description
Provides targeted funding for the advancement and application of health research knowledge to address priority health challenges identified by CIHR in collaboration with other federal departments and agencies, other national governments and non-governmental or private sector organizations. Funds may be used to cover research project expenditures as well as salaries or consultation fees. Targeted health challenges currently include: HIV/AIDS Initiative; National Anti-Drug Strategy (NADS); Drug Safety and Effectiveness Network (DSEN); and Networks of Centres of Excellence (which includes the NCE program, Business-led NCEs and Centres of Excellence for Commercialization and Research).
| 2014–15 Planned Spending |
2014–15 Actual Spending |
2014–15 Difference (actual minus planned) |
|---|---|---|
65,997,459 |
78,574,936 |
12,577,477 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
21 |
24 |
3 |
| Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
Government and external stakeholders invest in horizontal health research initiatives |
Ratio of leveraged funds for horizontal health research initiatives |
$1 : $0.60 |
$1 : $0.66 This result shows a slight increase in the ratio of leveraged funds from 2013−14. The increase is due, in part, to a change in the methodology used to capture partner investments. The methodology for future targets will be revised to reflect this change. |
Horizontal initiative research results in knowledge translation |
Percent of horizontal initiative grants reporting translation of knowledge |
Baseline Year |
73% of horizontal initiative grants reported translating knowledge. Trend analysis is not possible due to a lack of available historical data. |
CIHR-funded research findings contribute to more effective health services and products |
Percent of CIHR grants reporting contributions to more effective health services and products |
30% |
CIHR exceeded the target for 2014–15 by supporting grants of which 54% reported having contributed to more effective health services and products. This result is due, in part, to the dramatic increase in the data available for this fiscal year compared to previous years as the Research Reporting System brings more and more programs online and results are received. |
Performance Analysis and Lessons Learned
For more information on the variance between planned and actual spending and human resources, please see the section on the Priority-Driven Health Research program.
Through the Horizontal Health Research Initiatives sub-program, CIHR continued to provide funding and partner with key stakeholders to address horizontal health issues. Through DSEN, CIHR communicated the results of 21 DSEN queries regarding specific requests for drug safety and effectiveness evidence to federal regulators or federal/provincial decision makers. Another 23 queries are currently under research. DSEN has also developed DSEN Abstracts, which are high-level summaries of key findings, to disseminate research results to Canadians. Eight are presently available and other completed projects will also be provided once finalized.
In 2014–15, the DSEN program underwent an evaluation. The reception to the launch of DSEN’s new knowledge translation strategy demonstrated the value that regulators, decision-makers and researchers place on DSEN-generated research in increasing the impact on the health and safety of Canadians.
CIHR also invested $37.8M in the NCE suite of programs, including $12.0M for the CECR program, $22.5M for the NCE and $3.1M for Business-led NCEs. These investments build strong multisectoral linkages between academia, NGOs, government and industry, to accelerate research results for economic, social and environmental benefit. These results are consistent with the numbers for 2013−14, which show a total investment of $39.0M that year.
In the fall of 2014, as part of the National Anti-Drug Strategy (NADS), CIHR launched the Node Grant funding opportunity, second phase of the Canadian Research Initiative in Substance Misuse (CRISM). The objective of this funding opportunity was to establish regional nodes composed of researchers, service providers and representatives of people living with substance misuse, with shared infrastructure to facilitate research in interventions and other therapeutic approaches to substance misuse. Through this funding opportunity, four nodes were funded; one in Ontario, one in Quebec (which includes the Maritime Provinces), one in Alberta (which includes the other Prairie Provinces), and one in British Columbia. Each node is receiving $0.35M per year for five years.
Internal Services
Description
Internal Services are groups of related activities and resources that are administered to support the needs of programs and other corporate obligations of an organization. These groups are: Management and Oversight Services; Communications Services; Legal Services; Human Resources Management Services; Financial Management Services; Information Management Services; Information Technology Services; Real Property Services; Materiel Services; Acquisition Services; and Other Administrative Services. Internal Services include only those activities and resources that apply across an organization and not to those provided specifically to a program.
| 2014–15 Main Estimates |
2014–15 Planned Spending |
2014–15 Total Authorities Available for Use |
2014–15 Actual Spending (authorities used) |
2014–15 Difference (actual minus planned) |
|---|---|---|---|---|
3,019,312 |
3,231,910 |
3,306,303 |
3,284,376 |
52,466 |
| 2014–15 Planned |
2014–15 Actual |
2014–15 Difference (actual minus planned) |
|---|---|---|
23 |
23 |
0 |
Performance Analysis and Lessons Learned
As part of CIHR’s new strategic plan for 2014–15 – 2018–19, Health Research Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians (Roadmap II) released on March 11, 2015, CIHR recommitted to organizational excellence. As part of the new strategic plan, CIHR implemented a new performance measurement regime toolbox which aligns performance measures, expected outcomes and targets across all levels of the organization. This toolbox improves CIHR reporting of achievements and their impact on the health care system and the health of Canadians.
In 2014–15, CIHR also developed and implemented a new multi-year investment planning process which supports sound financial and risk management practices. This new framework enables governance bodies to focus on CIHR’s proposed health research relevance and impact while using business processes that are clear, nimble, transparent, sustainable and flexible.
As part of larger Government of Canada commitments, CIHR completed its implementation of GCDocs across the organization using a functional based classification approach as well as establishing proper retention and disposition schedules for all information saved. CIHR also conducted a requirement analysis to implement TBS’s Standard on Email Management as part of the Government of Canada Email Management Initiatives and developed an implementation plan within TBS deadlines. Finally, using CIHR’s Enterprise Architecture Framework created in November 2013, a detailed enterprise architecture was completed for the Reforms of the Open Suite of programs and peer review processes in 2014–15; work is ongoing to complete a detailed enterprise architecture for the remainder of CIHR’s programs.
As CIHR implemented the performance measurement regime over the past year, a key finding of the process was the consistent need for common measures across provincial, national and international research funders. As a result, CIHR, along with the Michael Smith Foundation in British Columbia, is co-chairing the Canadian Health Services and Policy Research Alliance Impact Work Group, and participating in the Heads of International Research Organizations Forum to develop common data, metric and monitoring standards to better demonstrate the impacts of research investments.
Section III: Supplementary Information
Financial Statements Highlights
| Financial Information | 2014–15 Planned Results |
2014–15 Actual |
2013–14 Actual |
Difference (2014–15 actual minus 2014–15 planned) |
Difference (2014–15 actual minus 2013–14 actual) |
|---|---|---|---|---|---|
Total expenses |
999,367,000 |
1,027,717,000 |
1,008,884,000 |
28,350,000 |
18,833,000 |
Total revenues |
9,700,000 |
7,618,000 |
6,854,000 |
-2,082,000 |
764,000 |
Net cost of operations before government funding and transfers |
989,667,000 |
1,020,099,000 |
1,002,030,000 |
30,432,000 |
18,069,000 |
Total expenses were approximately $28.4 M higher than planned, due primarily to additional funding announced in Budget 2014 for CIHR’s SPOR, CCNA and Emerging Threats Health Research Initiatives, as well as the CECR/BL-NCE funds approved in Supplementary Estimates (which were unknown at the time that 2014–15 planned spending was determined). Total revenues fluctuate annually as they depend exclusively on the timing of receiving partner funding and disbursing that partner funding to health researchers.
Higher than planned total expenses of $28.4M in 2014–15 and lower than planned total revenues of approximately $2.1M resulted in net cost of operations before government funding and transfers being approximately $30.4 M higher than planned for the fiscal year. However, net cost of operations before government funding and transfers increased by only $18.1M (or 1.8%) over the prior fiscal year, as CIHR’s operations are very consistent on a year-over-year basis.
| Financial Information | 2014–15 | 2013–14 | Difference (2014–15 minus 2013-14) |
|---|---|---|---|
Total net liabilities |
15,017,000 |
14,395,000 |
622,000 |
Total net financial assets |
12,130,000 |
11,196,000 |
934,000 |
Departmental net debt |
2,887,000 |
3,199,000 |
-312,000 |
Total non-financial assets |
1,039,000 |
996,000 |
43,000 |
Departmental net financial position |
-1,848,000 |
-2,203,000 |
355,000 |
Total net liabilities of $15.0M and total net financial assets of $12.1M both increased in 2014–15 compared to the prior fiscal year due to an increase in Accounts Payable and Accrued Liabilities, resulting from the Government’s implementation of salary payments in arrears during the fiscal year. CIHR’s total departmental net debt as at March 31, 2015 did not materially change compared to the prior fiscal year. Total non-financial assets of $1.0M as at March 31, 2015 are also consistent with the prior fiscal year. As a result, CIHR’s departmental net financial position did not change materially compared to the prior fiscal year.
Financial Statements
CIHR's 2014–15 audited financial statements can be found on the CIHR website and form an integral part of the annual report. Included with this year's audited financial statements are the:
- Financial Statement Discussion and Analysis;
- Auditor's Report and Financial Statements (including the Statement of Management Responsibility Including Internal Control over Financial Reporting); and
- Annex: Summary of the Assessment of Effectiveness of the Systems of Internal Control over Financial Reporting and the Action Plan of the Canadian Institutes of Health Research for the Fiscal Year 2012–13 (Unaudited).
Supplementary Information Tables
The supplementary information tables listed in the 2014–15 Departmental Performance Report can be found on the Canadian Institutes of Health Research’s website.
- Departmental Sustainable Development Strategy;
- Details on Transfer Payment Programs of $5 Million or More; and
- Internal Audits and Evaluations.
Tax Expenditures and Evaluations
The tax system can be used to achieve public policy objectives through the application of special measures such as low tax rates, exemptions, deductions, deferrals and credits. The Department of Finance Canada publishes cost estimates and projections for these measures annually in the Tax Expenditures and EvaluationsFootnote 41 publication. The tax measures presented in the Tax Expenditures and Evaluations publication are the sole responsibility of the Minister of Finance.
Section IV: Organizational Contact Information
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
Canada
Telephone: 613-941-2672
Fax: 613-954-1800
Appendix: Definitions
Appropriation: Any authority of Parliament to pay money out of the Consolidated Revenue Fund.
Budgetary expenditures: Include operating and capital expenditures; transfer payments to other levels of government, organizations or individuals; and payments to Crown corporations.
Departmental Performance Report: Reports on an appropriated organization’s actual accomplishments against the plans, priorities and expected results set out in the corresponding Reports on Plans and Priorities. These reports are tabled in Parliament in the fall.
Full-time equivalent: Is a measure of the extent to which an employee represents a full person-year charge against a departmental budget. Full-time equivalents are calculated as a ratio of assigned hours of work to scheduled hours of work. Scheduled hours of work are set out in collective agreements.
Government of Canada outcomes: A set of 16 high-level objectives defined for the government as a whole, grouped in four spending areas: economic affairs, social affairs, international affairs and government affairs.
Management, Resources and Results Structure: A comprehensive framework that consists of an organization’s inventory of programs, resources, results, performance indicators and governance information. Programs and results are depicted in their hierarchical relationship to each other and to the Strategic Outcome(s) to which they contribute. The Management, Resources and Results Structure is developed from the Program Alignment Architecture.
Non-budgetary expenditures: Include net outlays and receipts related to loans, investments and advances, which change the composition of the financial assets of the Government of Canada.
Performance: What an organization did with its resources to achieve its results, how well those results compare to what the organization intended to achieve and how well lessons learned have been identified.
Performance indicator: A qualitative or quantitative means of measuring an output or outcome, with the intention of gauging the performance of an organization, program, policy or initiative respecting expected results.
Performance reporting: The process of communicating evidence-based performance information. Performance reporting supports decision making, accountability and transparency.
Planned spending: For Reports on Plans and Priorities (RPPs) and Departmental Performance Reports (DPRs), planned spending refers to those amounts that receive Treasury Board approval by February 1. Therefore, planned spending may include amounts incremental to planned expenditures presented in the Main Estimates.
A department is expected to be aware of the authorities that it has sought and received. The determination of planned spending is a departmental responsibility, and departments must be able to defend the expenditure and accrual numbers presented in their RPPs and DPRs.
Plans: The articulation of strategic choices, which provides information on how an organization intends to achieve its priorities and associated results. Generally a plan will explain the logic behind the strategies chosen and tend to focus on actions that lead up to the expected result.
Priorities: Plans or projects that an organization has chosen to focus and report on during the planning period. Priorities represent the things that are most important or what must be done first to support the achievement of the desired Strategic Outcome(s).
Program: A group of related resource inputs and activities that are managed to meet specific needs and to achieve intended results and that are treated as a budgetary unit.
Results: An external consequence attributed, in part, to an organization, policy, program or initiative. Results are not within the control of a single organization, policy, program or initiative; instead they are within the area of the organization’s influence.
Program Alignment Architecture: A structured inventory of an organization’s programs depicting the hierarchical relationship between programs and the Strategic Outcome(s) to which they contribute.
Report on Plans and Priorities: Provides information on the plans and expected performance of appropriated organizations over a three-year period. These reports are tabled in Parliament each spring.
Strategic Outcome: A long-term and enduring benefit to Canadians that is linked to the organization’s mandate, vision and core functions.
Sunset program: A time-limited program that does not have an ongoing funding and policy authority. When the program is set to expire, a decision must be made whether to continue the program. In the case of a renewal, the decision specifies the scope, funding level and duration.
Target: A measurable performance or success level that an organization, program or initiative plans to achieve within a specified time period. Targets can be either quantitative or qualitative.
Whole-of-government framework: Maps the financial contributions of federal organizations receiving appropriations by aligning their Programs to a set of 16 government-wide, high-level outcome areas, grouped under four spending areas.
- Date modified: