2016–17 Departmental Results Report
Table of contents
- Minister's message
- Results at a glance
- Raison d'être, mandate and role: who we are and what we do
- Operating context and key risks
- Results: what we achieved
- Analysis of trends in spending and human resources
- Supplementary information
- Appendix: definitions
Minister's message

I am pleased to present the 2016–17 Departmental Results Report of the Canadian Institutes of Health Research (CIHR).
In 2016–17, CIHR continued to work closely with Canada's health research community to assess the process by which research grant applications are funded and adjudicated. Through an ongoing dialogue with leaders across all pillars of health research, CIHR continues to make improvements aimed at ensuring the quality, integrity, and sustainability of Canada's health research funding system and peer review process. We wish to thank Canada's health research community for their input and engagement in this important issue.
This year, CIHR also made significant advances toward improving the health and well-being of Indigenous populations. Consistent with a number of the calls to action of the Truth and Reconciliation Commission of Canada, and in consultation with First Nations, Inuit, and Métis communities, CIHR committed to implementing a series of concrete actions to further strengthen Indigenous health research in Canada. Most notably, CIHR committed to increasing its investments in Indigenous health research to a minimum of 4.6% (proportional to Canada's Indigenous population) of CIHR's annual budget.
Through Canada's Strategy for Patient-Oriented Research, CIHR continues to work collaboratively with patients, researchers, health care professionals, provinces and territories, and other key partners to help move research evidence into health system policy and clinical practice. This year, three new SUPPORT Units were implemented in British Columbia, Saskatchewan, and the Northwest Territories. These centres of expertise in patient-oriented research will be connected with similar centres located throughout Canada, allowing the provinces and territories to share best practices and accelerate research evidence into care.
Health research is one of the most important investments we can make as a nation, and CIHR plays an integral role in supporting our country's best and brightest researchers. I invite you to read this report to learn more about how CIHR is creating new knowledge and translating it into improved health, more effective health services and products, and a strengthened Canadian health care system.
The Honourable Ginette Petitpas Taylor, P.C., M.P.
Minister of Health
Results at a glance
In 2016–17, CIHR spent a total of $1,081.3M and engaged 425 employees to deliver on its mandate. This investment supported health research to improve the health of Canadians and the effectiveness of the health care services provided to Canadians.
| 2016–17 Results HighlightsFootnote * | 2016–17 Actual FTEs |
2016–17 Actual spendingFootnote ** (dollars) |
|---|---|---|
| Operating Support: CIHR is committed to discovery-oriented, investigator-led research and spends over half of its budget to support research programs and projects identified by scientists across the country. In Budget 2016, the Government of Canada provided CIHR with an additional $30.0M per year. These funds were directed to supporting Investigator-Initiated Research among Early Career Investigators. CIHR funded a total of 3,394 new and ongoing grants in areas identified by health researchers for a total investment of $539.1M in 2016–17. This funding represents the second consecutive year of growth in CIHR investment; the total investment in this Sub-program represents a $19.5M increase from 2015–16. CIHR continued to integrate its legacy open programs into the new Foundation Grant and Project Grant programs. CIHR also established the College of Reviewers to create a national resource that facilitates peer review across Canada, in all areas of health research. | 81 | 547,703,924 |
| Training and Career Support: By investing in the next generation of researchers, CIHR ensures that the Canadian health research enterprise has the capacity to respond to new or existing health challenges in Canada and throughout the world. In 2016–17, through the Training and Career Support Sub-program, CIHR directly provided 2,305 new and ongoing training and salary awards for a total investment of $159.5M, which is just under the 2015–16 investment of $160.8M. | 36 | 162,519,017 |
| Institute-Driven Initiatives: CIHR's 13 Institutes promote and build upon Canada's firm foundation of research excellence. They engage the research community and encourage interdisciplinary, integrative health research to address gaps or emerging health priorities. The Institute-Driven Initiative Sub-program provides targeted grants and awards funding to accelerate and mobilize, in an ethical manner, Canada's health research community to work together to address priority health challenges. In 2016–17, CIHR invested $228.3M through 1,808 grants and awards, of which 1,117 were new. This fiscal year, the total investment in this Sub-program is higher than the 2015–16 investment by $27.4M. | 81 | 238,048,994 |
| Horizontal Health Research Initiatives: CIHR, through the Horizontal Health Research Initiatives Sub-program, provides targeted funding for the advancement and creation of new knowledge and its translation into improved health for Canadians, more effective health services and products, and a strengthened Canadian health care system. This Sub-program addresses priorities identified by CIHR in collaboration with other federal departments or agencies, other national governments, non-governmental organizations, or private sector organizations. In 2016–17, CIHR increased its investment to $97.4M through 229 new and ongoing grants and awards, of which 101 were new. This investment is higher than in 2015–16 by $5.9M. | 29 | 101,220,192 |
For more information on the Canadian Institutes of Health Research's plans, priorities and results achieved, see the "Results: what we achieved" section of this report.
Raison d'être, mandate and role: who we are and what we do
Raison d'être
CIHR Institutes
Scientific Directors
Aboriginal Peoples' Health
Dr. Carrie Bourassa
Aging
Dr. Yves Joanette
Cancer Research
Dr. Stephen Robbins
Circulatory and Respiratory Health
Dr. Brian H. Rowe
Gender and Health
Dr. Cara Tannenbaum
Genetics
Dr. Paul Lasko
Health Services and Policy Research
Dr. Robyn Tamblyn
Human Development, Child and Youth Health
Dr. Shoo K. Lee
Infection and Immunity
Dr. Marc Ouellette
Musculoskeletal Health and Arthritis
Dr. Hani El-Gabalawy
Neurosciences, Mental Health and Addiction
Dr. Samuel Weiss
Nutrition, Metabolism and Diabetes
Dr. Philip M. Sherman
Population and Public Health
Dr. Steven J. Hoffman
Canadian Institutes of Health Research (CIHR) is the Government of Canada's health research funding agency. The Minister of Health is responsible for this organization. It was created in June 2000 by the Canadian Institutes of Health Research Act with a mandate "to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system."
CIHR's mandate seeks to transform health research in Canada, in an ethically sound manner, by:
- Funding both investigator-initiated and priority-driven research;
- Building research capacity in under-developed areas and training the next generation of health researchers; and
- Focusing on knowledge translation that facilitates the application of the results of research and their transformation into new policies, practices, procedures, products and services.
Mandate and role
CIHR integrates research through a unique interdisciplinary structure made up of 13 "virtual" institutes. These institutes are not "bricks and mortar" buildings but communities of experts in specific areas. Collectively, the institutes support a broad spectrum of research: biomedical; clinical; health systems and services; and the social, cultural and environmental factors that affect the health of populations. Institutes form national research networks linking researchers, funders and knowledge users across Canada to work on priority areas.
CIHR makes an essential contribution to the Minister of Health's overall responsibilities by funding the research and knowledge translation needed to inform the evolution of Canadian health policy and regulation, and by taking an advisory role on research and innovation issues. This is achieved through an extensive and growing set of linkages with Health Canada and the Public Health Agency of Canada, providing decision makers with access to high-quality and timely health research outcomes/results.
CIHR also works closely with the Natural Sciences and Engineering Research Council (NSERC) and the Social Sciences and Humanities Research Council (SSHRC), the two granting councils of the Innovation, Science and Economic Development Portfolio. This work ensures that the organizations share information and coordinate efforts, harmonize practices, avoid duplication and foster multidisciplinary research. The three organizations (referred to as "Tri-Agency") provide a channel for the implementation of common policies, practices and approaches, whenever possible.
CIHR's Governing Council (GC) sets the strategic direction of the Agency and is responsible for evaluating its performance. Leadership on research, knowledge translation and funding for research is provided by the Science Council (SC), while leadership on corporate policy and management is provided by the Executive Management Committee (EMC).
For more general information about the department, see the "Supplementary information" section of this report. For more information on the department's organizational mandate letter commitments, see the Minister's mandate letter.
Operating context and key risks
Operating context
Over the past several years, CIHR has been adapting to meet the challenges of a rapidly evolving and increasingly complex health research landscape. To address this shifting context, CIHR has been implementing its strategic plan (Roadmap II) to enable CIHR to carry out its full mandate, demonstrate a capacity for leadership within the wider health research community, and ensure accountability and results to Canadians.
In 2016, CIHR launched its first Project Grant competition as part of the major reforms of its Investigator-Initiated Health Research Program and peer review processes. These reforms were intended to contribute to a sustainable Canadian health research enterprise by supporting world-class researchers in the conduct of research and its translation across the full spectrum of health, and to ensure the reliability, consistency, fairness and efficiency of the competition and peer review processes. However, in practice, CIHR faced several challenges with the implementation of these changes, particularly with respect to the online peer review process.
Scientists across Canada publicly voiced concerns with the peer review process of the 2016 Project Grant competition, and called on CIHR to make changes to those processes. On July 5, 2016, the Minister of Health, the Honourable Jane Philpott, issued a statement noting the growing concerns of the health research community and requesting that CIHR convene a Working Meeting with key representatives of the research community to find common ground and move forward with solutions to address the issues raised with regard to the quality and integrity of CIHR's peer review system. CIHR convened this meeting on July 13, 2016 in Ottawa.
As a follow-up to this Working Meeting, a Peer Review Working Group was established. This group developed a list of recommendations to strengthen the peer review processes of CIHR's Project Grant program. This work continues through engagement with the College of Reviewers and other stakeholders (e.g., University Delegates) and these recommendations may be implemented in future competitions. The recommendations included reviewing all Indigenous health research applications through an iterative peer review process and equalizing the success rate for early career investigators (ECIs) (the proportion of ECIs funded equals the proportion of ECI applicants to the competition), both of which are being implemented.
In September 2016, CIHR launched the International Peer Review Expert Panel. This Panel was chaired by the Chief Scientific Advisor to the Prime Minister of New Zealand and included six other international leaders in health science and science funding. The Panel assessed the design and implementation of CIHR's new grants adjudication processes and their work was informed by consultation with the scientific community, the Scientific Directors of CIHR's thirteen Institutes, partners, and members of the CIHR Peer Review Working Group. In February 2017, the Panel's final report was tabled and accepted by CIHR's Governing Council, and made public. The report included a number of observations about CIHR and peer review practices and offered nine recommendations for action. CIHR continues to work on a management response to the report with stakeholder input and given the evolving landscape of its peer review processes.
On November 4, 2016, CIHR's former President, Dr. Alain Beaudet, announced at the National Forum on the 20th Anniversary of the Royal Commission on Aboriginal Peoples an Action Plan: Building a healthier future for First Nations, Inuit, and Métis Peoples. With this plan, CIHR is reiterating its commitment to strengthen its relationship with First Nations, Inuit and Métis Peoples and identifying concrete actions to support Indigenous health research in Canada, with the aim of improving Indigenous health outcomes. In 2016–17, CIHR began to implement a series of concrete actions to further strengthen Indigenous health research, including the commitment to increase its investments in Indigenous health research to a minimum of 4.6% of its annual budget.
Key risks
The risks identified in the tables below are from CIHR's 2016–17 Corporate Risk Profile, which identified five risks requiring mitigation and monitoring to ensure the associated response strategies reduce the impact of the risk. The three highest risks are outlined in the tables below along with their associated Risk Response Strategy.
Key risks
| Risk 1 – CIHR's current commitments to our priorities may result in unsustainable pressure on available resources | Mitigating strategy and effectiveness | Link to the department's Programs | Link to mandate letter commitments or to government-wide and departmental priorities |
|---|---|---|---|
|
Given the current limited available resources – both Grants and Awards and operational funding – there is a risk that CIHR's ability to remain responsive and adaptable within a rapidly changing health research environment will be limited. As a result, CIHR would have reduced operational capacity to effectively invest in new high-impact health research, while sustaining investments in Investigator-Initiated research. Furthermore, there are limited available resources as noted in Risk 3. |
This risk was identified in both the 2016–17 RPP and the 2016–17 Corporate Risk Profile (CRP). CIHR responded to this risk by:
This risk will continue to be monitored in 2017–18. |
|
Government-wide priority:
CIHR Priorities:
|
| Risk 2 – Maintaining ongoing business and supporting new business processes. | Mitigating strategy and effectiveness | Link to the department's Programs | Link to mandate letter commitments or to government-wide and departmental priorities |
|---|---|---|---|
Limitations and delays in technology modernization and integration may impact CIHR's ability to adequately maintain our ongoing business as well as support new business processes. |
This risk was identified in both the 2016–17 RPP and the 2016–17 CRP. CIHR responded to this risk by:
This risk will continue to be monitored in 2017–18. |
|
Government-wide priority:
CIHR Priorities:
|
| Risk 3 – CIHR's reputation, external support and stakeholder engagement are being impacted due to significant change within the Agency | Mitigating strategy and effectiveness | Link to the department's Programs | Link to mandate letter commitments or to government-wide and departmental priorities |
|---|---|---|---|
Given recent multiple changes occurring simultaneously at CIHR, there is a risk that desired outcomes will be misunderstood both within CIHR and the research community, thus leading to disengagement and limiting the ability to enact the desired transformations. Furthermore, the level of complexity of these transformations along with limited available resources raise the level of impact of this risk. |
This risk was identified in both the 2016–17 RPP and the 2016–17 CRP. CIHR responded to this risk by:
This risk will continue to be monitored in 2017–18. |
|
Government-wide priority:
CIHR Priorities:
|
CIHR strives for innovation in how it conducts its business and in how it responds to Government of Canada priorities and commitments. In 2016–17, CIHR applied solutions to its technology infrastructure in order to improve client service and reduce complexity for stakeholders. A major accomplishment was the scale-up of a single point of entry system for stakeholder enquiries – the CIHR Contact Centre. The Contact Centre manages and tracks all enquiries into CIHR and manages them through a service standard designed to ensure prompt service and high quality responses. CIHR increased the quality, efficiency and effectiveness of this system by monitoring service standards and reporting on them quarterly.
In 2016–17, CIHR continued its information technology and systems modernization and integration efforts by establishing the Enabling Business by Leveraging Systems (EnaBLeS) project. EnaBLeS outlines technology-enabled business processes and solutions which will strengthen CIHR's collaboration with stakeholders, facilitate high-quality peer review, and improve the efficiency and effectiveness of CIHR's services and operations, including learning management. CIHR piloted technology to support automation and greater efficiency of matching applications to reviewers. The software was also intended to assist in identifying new areas of expertise in a larger pool of reviewers. Though the software is no longer being used for this full purpose, systems modernization remains a CIHR priority. Over the course of the year, preliminary work to define the scope of the project, develop the project charter and outline as implementation process to ensure the success of the 4.5-year project was initiated.
CIHR also began the development of a new partnership strategy to bring a focus to partner engagement, explore new models for partnership, and deliver greater impact, for the benefit of Canadians. Stakeholder and partner consultations on the new strategy were completed this year.
Results: what we achieved
CIHR is the Government of Canada's health research investment agency. Overall, in 2016–17, CIHR supported more than 12,800 researchers and trainees in the fulfillment of its mission: to create new scientific knowledge and to enable its translation into improved health, more effective health services and products, and a strengthened Canadian health care system.
CIHR is guided by a peer review system that supports the selection of the most innovative and cutting-edge proposals for research and/or knowledge translation, while upholding the principles of fairness and transparency. In 2016–17, approximately 3,600 peer reviewers provided their time, without remuneration, to review over 10,400 applications.
CIHR's strategic plan, Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians, strikes a balance between completing the transformation envisioned and initiating new priorities, and is fully aligned to the Program Alignment Architecture.
Specifically, CIHR supports research through the following programs:
- Investigator-Initiated Health Research; and
- Priority-Driven Health Research.
Both programs are supported by Internal Services.
Research in Action: Improving Lung Transplantation
The Ex Vivo Lung Perfusion (EVLP) system – named one of "Five Discoveries that Will Change the Future of Organ Transplants" (Time.com, June 2013) – was developed by Dr. Shaf Keshavjee (O.C.) and his team at the University Health Network (UHN). EVLP enables clinicians to preserve donor lungs for assessment for up to six hours prior to transplant, during which time there is the potential for supported lung repair. This allows for healthier donor lungs for transplantation, reduced wait times, and reduced post-transplant complications and costs typically associated with the use of injured donor lungs. At UHN, donor lung utilization has increased from 15% to 35%, with similar utilization rates reported by major transplant centres worldwide. Health Canada has approved EVLP for clinical transplantation and endorses reimbursement of the associated costs. The research team serves as the official guideline author on EVLP for the Food and Drug Administration in the United States, and has created an ex vivo perfusion industry through spin-off companies in Canada and the US. These companies are developing the next generation of perfusion systems and acting as a skilled service provider of ex vivo organ assessment and rehabilitation.
Distribution of 2016–17 Actual Spending by Program
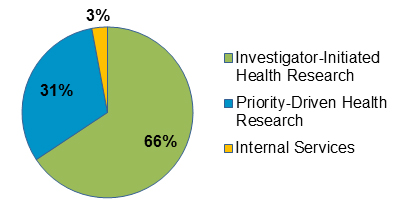
Figure 1 long description
| Investigator-Initiated Health Research | Priority-Driven Health Research | Internal Services |
|---|---|---|
| 66% | 31% | 3% |
Distribution of 2016–17 Actual FTEs by Program
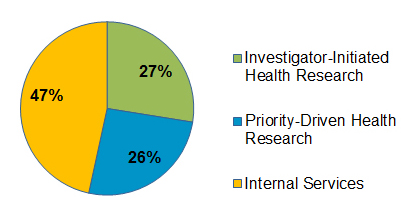
Figure 2 long description
| Investigator-Initiated Health Research | Priority-Driven Health Research | Internal Services |
|---|---|---|
| 27% | 26% | 47% |
Programs
Program 1.1: Investigator-Initiated Health Research
Description
To develop and support a well-trained base of world-class health researchers and trainees conducting ethically sound research across all aspects of health, including biomedical research, clinical research, research respecting health systems, health services, the health of populations, societal and cultural dimensions of health and environmental influences on health, and other research as required. The goal of this program is to advance health knowledge and to apply this knowledge in order to improve health systems and/or health outcomes. Grants and awards are disbursed to fund research or to provide career or training support. The specific area of research is identified by the researcher.
Results
Results Highlights
In 2016–17, CIHR:
- Invested a total of $698.6M in all facets of health research through Investigator-Initiated Health Research grants and awards.
- Awarded 954 new training and salary awards through the Sub-program Training and Career Support for a total investment of $35.8M.
- Completed two evaluations under this Program – the Canada Graduate Scholarship (CGS) program and Strategic Training Initiative in Health Research (STIHR).
CIHR's Investigator-Initiated Health Research Program is composed of two Sub-programs: Operating Support, and Training and Career Support. Investigator-Initiated Health Research funding plays an important role by allowing researchers to identify the area of research they wish to pursue, and providing support for the very best ideas, from discovery to application. It also provides opportunities to train the next generation of health researchers and professionals.
In 2016–17, CIHR continued to develop and support a well-trained base of world-class health researchers and trainees. This occurred by funding a total of 5,699 grants and awards. This result is below the target total of 6,000 grants and awards set out in the 2016–17 Report on Plans and Priorities, but surpassed its expected 1,500 new grants and awards (actual result was 1,724 new grants and awards).
All investigator-initiated health research at CIHR undergoes peer review prior to funding. An exciting development in 2016–17 was the broader implementation of the College of Reviewers with the research community. CIHR appointed 16 College Chairs and one Executive Chair. The inaugural slate of College Chairs is comprised of leading, senior researchers whose expertise and experience spans CIHR's health research and knowledge translation mandate. The role of the College Chairs is to ensure that the peer review system supports the selection of the most innovative and cutting-edge proposals for research and knowledge translation, while continuing to be fair, well-managed and transparent.
As part of CIHR's new peer review processes and activities, a reviewer profile to support the matching of applications to reviewers was created and implemented. With the oversight of the College Chairs, an observer program for ECIs and a new review quality assurance process were also piloted in the fall 2016 Project Grant competition. These activities will support mentorship of the next generation of peer reviewers and will also support high quality peer review now and into the future.
Operating Support Sub-program
Research in Action: Improving the Treatment of Type 2 Diabetes
In 2007, a CIHR Team Grant was awarded to the Alliance for Canadian Health Outcomes Research in Diabetes (ACHORD) – five Alberta researchers studying the impact of diabetes on Canadians. The purpose of this grant was three-fold: to develop research capacity in this field, to broaden our understanding of the burden of diabetes, and to improve the quality of care. Examination of administrative data from Saskatchewan revealed that patients who used metformin were less likely to be hospitalized or die compared to those who used other diabetes medications. These research findings were incorporated into the Canadian Diabetes Association's 2008 clinical practice guideline, which specified that metformin is a safe and effective treatment for patients with diabetes and heart failure. This policy change has resulted in a significant impact on clinical practice for Canadians with Type 2 diabetes.
In 2016–17, CIHR continued to implement the Foundation Grant and Project Grant Programs – the two main programs through which CIHR funds Investigator-Initiated Health Research. CIHR announced the results of the second Foundation Grant competition, which included 120 new research programs for a total of $292M, which represents 33 new/early career investigators supported for five years and 87 mid-career/senior investigators supported for seven years.
In 2016–17, CIHR completed two Project Grant competitions. The first pilot Project Grant competition supported 491 research grants across all four areas of health research, plus an additional 127 one-year bridge grants, for an announced investment of approximately $376M. An additional specific annual and ongoing funding envelope of $30M was dedicated to research projects from ECIs, as part of a Governing Council decision in response to the 2016 Federal Budget investment for investigator-initiated research. This dedicated funding provided support for an additional 40 research projects from ECIs, bringing the total number of fully funded projects for applicants in this career stage from 58 to 98.
The second Project Grant competition (fall 2016) announced support for an additional 475 research grants and 121 one-year bridge grants, for a total investment of approximately $359M. The 475 grants approved were awarded to 461 investigators (14 investigators were awarded two grants) and 108 new/early career investigators. All Indigenous health research applications went through an iterative peer review process. Based on the recommendation of the Indigenous health research peer review cluster, 22 of the 475 grants and 12 of the 121 one-year bridge grants were awarded to Indigenous health research projects.
Training and Career Support Sub-program
Research in Action: Improving Cardiac and Stroke Care
As a CIHR Industry Partnered Research Chair, Dr. Anthony Tang established a national mentoring program for young researchers in clinical electrophysiology. He led a research program demonstrating that combining cardiac resynchronization therapy (CRT) and an Implantable Cardioverter Defibrillator (ICD) can reduce mortality and morbidity; and investigated therapies for heart failure and atrial fibrillation in an effort to reduce cardiac deaths. Through the CIHR University Industry Program, together with Medtronic, Dr. Tang led the large multi-centre clinical trial Resynchronization/Defibrillation for Ambulatory Heart Failure Trial (RAFT). Building on his efforts, a CIHR funded Canadian Stroke Prevention Intervention Network (C-SPIN) was established to reduce the incidence of atrial fibrillation related stroke. Dr. Tang is now leading CANet (Cardiac Arrhythmia Network of Canada), funded by the Networks of Centres of Excellence of Canada program. This network aims to develop innovative solutions to improve quality, increase accessibility, and develop sustainable cost-effective arrhythmia care In Canada. The Network also seeks to recruit, train, support and retain clinical scientists.
In 2016–17, CIHR provided direct support to maintain Canada's ability to train, retain and sustain outstanding health researchers – a key priority of CIHR's five-year strategic plan. It achieved its commitments by funding 131 new Canada Graduate Scholarships (CGS) doctoral awards and 396 new CGS master's awards; 55 new three-year Vanier CGS; 23 new two-year Banting Postdoctoral Fellowship awards; and 160 new CIHR fellowships. These investments in supporting outstanding trainees from the Master's, Doctoral, and Post-doctoral levels are contributing to the pipeline of highly qualified personnel in Canada.
CIHR developed an End-of-Award Report for the Vanier program which will be sent to recipients, starting in 2017–18. Using performance measurement and evaluation best practices, this end-of-award reporting approach will produce high quality data that will allow CIHR to examine the impacts of this program.
In 2016–17, a second evaluation of the Canada Graduate Scholarship (CGS) program was conducted. The evaluation found the CGS program to be effective, relevant, and supportive of the development of highly qualified personnel, thereby helping to ensure that Canada's knowledge economy remains globally competitive well into the future. The evaluation identified the need to revise the CGS program's expected outcomes and strengthen performance measurement, as well as the need to provide more information on the review process and its outcomes to applicants. Details on the evaluation can be found on the CIHR website.
The second evaluation of the Strategic Training Initiative in Health Research (STIHR) was also completed in 2016–17. The evaluation found the Initiative to be effective and to have met its objectives. Given that CIHR is no longer launching open STIHR funding opportunities, recommendations focused on informing CIHR's Strategic Action Plan on Training (T-SAP) and future training initiatives. Details on the evaluation can be found on the CIHR website.
In 2016–17, CIHR funded 110 new awards through the Canada Research Chairs (CRC) program which included 40 new Tier 1 Chairs and 70 new Tier 2 Chairs. In total, CIHR invested $87.5M through the CRC program, supporting 643 emerging and established investigators.
In 2016–17, CIHR continued to support world-class research by funding seven applications through the Canada Excellence Research Chair Tri-Agency program, for a total of $9.8M.
| Expected results | Performance indicators | Target | Date to achieve target | 2016–17 Actual results | 2015–16 Actual results | 2014–15 Actual results |
|---|---|---|---|---|---|---|
| Canada has an internationally competitive health research community | Canada's health research specialization index ranking versus international levels (G7 nations) | 2nd among G7 nations | March 31, 2017 | In 2014 (last data available), Canada was ranked 2nd in the health research specialization index when compared to G7 nations. This is consistent with the 2015–16 Departmental Performance Report (DPR) result. | 2nd | 2nd |
| CIHR-funded research has improved the health of Canadians | Percent of CIHR Investigator-Initiated Health Research grants reporting contribution to improved health for Canadians | 33% | March 31, 2017 | CIHR met the 2016–17 target by supporting grants of which 37% reported contributing to improved health for Canadians. This is consistent with the 2015–16 DPR result of 37%. | 37% | 34% |
| Canadian health researchers advance health research knowledge | Canada's ranking among G7 in health research publications per million dollars of gross domestic expenditure on research and development (GERD) | 2nd among G7 nations | March 31, 2017 | In 2015 (last data available), Canada was ranked 1st among the G7 nations which is higher than previous years. | 1st | 3rd |
| 2016–17 Main Estimates |
2016–17 Planned spending |
2016–17 Total authorities available for use |
2016–17 Actual spending (authorities used) |
2016–17 Difference (actual minus planned) |
|---|---|---|---|---|
| 692,439,221 | 692,653,215 | 721,190,915 | 710,222,941 | 17,569,726 |
| 2016–17 Planned | 2016–17 Actual | 2016–17 Difference (actual minus planned) |
|---|---|---|
| 104 | 117 | 13 |
Information on CIHR's lower-level programs is available on the CIHR's website and in the TBS InfoBase.
Program 1.2: Priority-Driven Health Research
Description
CIHR provides funding to researchers for ethically sound emergent and targeted research that responds to the changing health needs and priorities of Canadians across all aspects of health, including biomedical research, clinical research, research respecting health systems, health services, the health of populations, societal and cultural dimensions of health and environmental influences on health, and other research as required. The goal of this program is to advance health knowledge and its application, in specific areas of research identified by CIHR in consultation with other government departments, partners and stakeholders, in order to improve health systems and/or improve health outcomes in these priority areas. Grants are disbursed to fund research or to provide career or training support.
Results
Results Highlights
In 2016–17, CIHR:
- Invested a total of $325.7M through the Priority-Driven Health Research Program, which is designed to fund grants and awards in emerging, priorities and future needs of health research.
- Completed an evaluation of the Strategy for Patient-Oriented Research.
Through this Program, CIHR provides targeted grant and award funding to mobilize researchers, health practitioners and decision makers to work together to address priority health challenges through two Sub-programs: Institute-Driven Initiatives and Horizontal Health Research Initiatives. In 2016–17, CIHR invested in 2,037 grants and awards through these initiatives, of which 1,278 were new. These results are slightly lower than the goal of 2,200 grants and awards, 1,300 new, outlined in the 2016–17 RPP, however, the total investment was higher than in 2015–16. The variance was a result of the alignment and modernization of various initiatives to bring together researchers through collaborations, large teams and networks (which resulted in fewer grants).
In 2016–17, CIHR continued to lead global health research initiatives in partnership with other health research funders. CIHR collaborated with the Bill & Melinda Gates Foundation by co-funding new HIV/AIDS research grants. These grants were designed to foster a culture of innovation in Canada by supporting innovative or high-risk biomedical and clinical projects with the potential for transformative advances in the area of HIV/AIDS. CIHR also launched a $15.0M program to address mental health disorders in China in collaboration with the National Natural Research Foundation of China and the Global Alliance for Chronic Diseases (GACD). This partnership with the GACD represents the fourth time that CIHR has joined forces with the Alliance to address priorities shared by Canada and the global community (the previous launches funded research in hypertension, Type 2 diabetes, and lung diseases).
In addition to addressing chronic diseases globally, CIHR used its Emerging Threats Initiative to co-invest $3.0M with the International Development Research Centre (IDRC) to fund teams of Canadian and Latin American and Caribbean researchers. CIHR also partnered with IDRC through the Global Research Collaboration for Infectious Disease Preparedness which co-hosted a Zika research workshop in Brazil, bringing together research funders and researchers to discuss collaboration on harmonized research approaches to study the Zika virus.
Institute-Driven Initiatives Sub-program
In 2016–17, through the Institute-Driven Initiatives Sub-program, CIHR continued to address complex problems and create transformative and measurable impact through the support of existing/emerging Signature Initiatives and other major initiatives. At least one of the CIHR's 13 Institutes offers leadership for these Initiatives; the majority are led by multiple Institutes. These Initiatives are designed to investigate pressing health issues that are of strategic importance to our country.
In 2016–17, through the Healthy Life Trajectories Initiative, CIHR committed an investment of $7.6M, over five years, to fund cohort studies. The goal is to generate evidence that will inform national policy and decision-making in Canada related to the improvement of health and the prevention of non-communicable diseases, with an emphasis on obesity, cardiovascular disease and diabetes throughout the lifespan. CIHR selected three collaborative international teams in 2016: Canada-South Africa, Canada-China and Canada-India. In December 2016, CIHR co-convened a workshop with three other funders and the World Health Organization, which brought together the teams to harmonize how data collection is approached and measured. To further build Canadian capacity in this research area, a competition was launched for a Canadian Cohort designed to align with the existing international cohorts.
CIHR continued to support leading edge research on the role of DNA and environment interactions in human health and disease through the Canadian Epigenetics, Environment and Health Research Consortium initiative. In 2016–17, CIHR renewed funding for two innovation centres (British Columbia and Quebec) to map epigenomic changes related to human health and disease ($8.4M from CIHR, leveraged with other members of the genomics research enterprise in Canada). As well, Canadian epigenomics researchers were central in a major coordinated global scientific paper release in 2016, providing publicly-accessible data to help researchers worldwide advance understanding of disease processes and improve patient outcomes.
The Environments and Health Signature Initiative builds on Canadian strengths in interdisciplinary environments and health research. In 2016–17, nine teams were funded to study inter-sectoral health promotion or prevention strategies related to the environment, with an investment of $17.9M, over six years. CIHR also funded a consortium which is linking environmental and health data, with an investment of $4.2M, over four years. Finally, CIHR funded six teams with an investment of $2.6M, over three years, through the Joint Programing Initiative on Antimicrobial Resistance (JPIAMR) to study Antimicrobial Resistance (AMR) transmission and the environment.
As part of the AMR Initiative, CIHR committed an investment of $1.5M to fund five teams conducting research towards developing rapid AMR diagnostic tools. Through JPIAMR, CIHR also supported two working groups of experts responsible for producing transnational guidelines designed to enhance resource alignment and maximize existing and future efforts to combat AMR.
CIHR and its partners are committed to using research to contribute to the creation of better preventive health services and healthier communities for First Nations, Métis and Inuit peoples in Canada. In 2016–17, through the Pathways to Health Equity for Aboriginal Peoples Signature Initiative, CIHR invested a total of $4.3M, over three years, in seven Pathways Implementation Research Teams focused on suicide prevention (2), diabetes/obesity (2), tuberculosis (1) and oral health (2). As well, an annual gathering provided Pathways funded researchers and community partners with an opportunity to share best practices.
The CIHR Dementia Research Strategy (DRS) supports efforts to identify preventive, diagnostic and treatment approaches for Alzheimer's disease and other neurodegenerative diseases causing dementia, while focusing as well on care and social inclusion of people living with dementia (and their caregivers). Through the DRS, CIHR assures collaborative Canadian participation and leadership in world class research that is aligned with a coordinated and global agenda. The DRS includes both national and international research partnerships and collaborations and, in 2016–17, CIHR continued to play a leadership role by convening the European Union Joint Programme – Neurodegenerative Diseases organizations for the first time in Canada.
In 2016–17, CIHR partnered with the Social Sciences and Humanities Research Council (SSHRC) to co-invest in research projects examining innovative ways to improve the health and productivity of Canada's diverse and changing workforce. Through the Healthy and Productive Work Initiative, 20 Partnership Development Grants were funded totaling $3.0M ($2.0M CIHR; $1.0M SSHRC), as part of a first phase of investment. CIHR also convened these teams with non-academic leaders in this field in a workshop to prepare for larger grants in the next phase. Nine additional teams were funded ($0.65M) to attend a "Work Stress and Wellbeing Hackathon," an initiative designed to develop innovative, evidence-informed, gender-responsive and culturally-appropriate digital mental health solutions. These solutions are intended to foster the labour force participation of women, men and gender-diverse people at risk of or struggling with workplace stress or mental health injuries.
CIHR, through the eHealth Innovations Partnership Program, facilitates partnerships between technology industries, researchers, decision-makers and end-users such as patients/families and clinicians with the goal of creating innovative approaches to health care delivery that will improve outcomes and patient experiences. In 2016–17, CIHR and partners – including organizations from the private, public, and non-profit sectors – funded 22 projects: eight focused on youth mental health and 14 focused on seniors with complex care needs in their homes. CIHR is providing a total of $13.9M, over four years, to support these 22 projects. An additional $32.0M is being provided by partners.
Horizontal Health Research Initiatives Sub-program
Through the Horizontal Health Research Initiatives Sub-program, in 2016–17, CIHR focused on the priority health challenges identified in collaboration with other federal departments or agencies (and other national governments) to address horizontal health issues in various programs.
For example, one of the priorities of the CIHR HIV/AIDS and STBBI Research Initiative Strategic Plan (2015–2020) is to improve health outcomes for people living with HIV by supporting the development, uptake and evaluation of models of care and new ways to mobilize research evidence. The CIHR HIV/AIDS and STBBI Research Initiative and its partners have developed an Implementation Science initiative to address the gap that exists in the application of evidence into health policy and programs. In 2016–17, CIHR invested $1.35M to fund nine grants in implementation science focused on two complementary funding opportunities: Adaptation Grants and Implementation Grants. CIHR hosted a workshop in May 2016 with the successful teams, and launched a funding opportunity to fund five teams to scale up interventions, which represents a commitment of $10.0M, over five years.
In 2009, CIHR established the Drug Safety and Effectiveness Network (DSEN) in collaboration with Health Canada and other stakeholders. The purpose of DSEN is to increase the evidence on drug safety and effectiveness available to regulators, policy-makers, health care providers and patients; and to increase the capacity within Canada to undertake high-quality post-market research in this area. In 2016–17, CIHR communicated through DSEN the results of 22 queries addressing specific requests for drug safety and effectiveness evidence by decision-makers.
In 2016–17, CIHR continued to support the Strategy for Patient-Oriented Research (SPOR) and its core elements: SUPPORT Units, Research Networks, Capacity Development, Improving the Clinical Trials Environment, and Patient Engagement. In 2016–17, to address the growing challenge of chronic disease in Canada, CIHR, in collaboration with over 120 partners from a variety of sectors, continued to co-fund five SPOR Networks in Chronic Disease. The goal of the Networks is to translate existing and new knowledge into innovations that can produce positive change in the health care system, within five years. In addition, three new SUPPORT Units were co-funded this year by CIHR and its partners, and are now in various stages of implementation: British Columbia ($80.0M), Saskatchewan ($63.0M), and the Northwest Territories ($21.0M). These centres of expertise in patient-oriented research will be connected with similar centres located throughout Canada, allowing provincial/territorial health care systems to share best practices and accelerate the application of research evidence into care.
Research in Action: Rapid Research on Ebola Vaccine
In response to the 2013-2016 Ebola virus outbreak in West Africa, a vaccine for Zaire Ebola virus was evaluated in humans for the first time in Canada. Supported by CIHR and PHAC, the study provided the first fully validated data confirming the intermediate term safety, tolerability, and effectiveness of the vaccine. The study's success enabled the team to lead efforts towards a phase II clinical trial in immunocompromised patients to be conducted in Canada and select African countries. The long-term data generated on this Canadian vaccine will enhance worldwide collaborations leading to the licensing of Ebola vaccines that protect humans and control outbreaks.
The first evaluation of SPOR was conducted in 2016–17, which examined program relevance, design and delivery, and performance. As SPOR is still a relatively new initiative, the report focused on the implementation and progress of its core elements during its first five years: SUPPORT Units, Research Networks, Capacity Development, Improving the Clinical Trials Environment, and Patient Engagement. The evaluation found that SPOR is relevant, and that it is a leading force in meeting Canada's need for patient-oriented research and evidence-informed care. It also confirmed the importance of the investments made by CIHR and its partners in this initiative. However, the evaluation also noted that some improvements are required to further strengthen SPOR's design and delivery, such as developing a communications plan for moving beyond the initial five-year funding period to manage sustainability expectations for CIHR investments in SPOR.
CIHR has continued to support and collaborate with NSERC and SSHRC on a series of Tri-Agency programs, such as the Networks of Centres of Excellence (NCE) delivered by the NCE Secretariat, and managed by NSERC. In 2016–17, CIHR invested $36.5M in the NCE suite of programs: $22.6M for the NCE program (including NCE-Knowledge Mobilization, NCE-International Knowledge Translation Platforms and the Canada-India Research Centre of Excellence), $10.8M for the Centres of Excellence for Commercialization and Research program, and $3.1M for the Business-led NCE program.
CIHR also participated in the Canada First Research Excellence Fund (CFREF), a program administered by SSHRC on behalf of the Tri-Agency. CFREF is designed to provide funding to Canada's post-secondary institutions to position them to compete with the best in the world for talent, partnership opportunities and breakthrough discoveries, thus creating long-term economic advantages for Canada. In 2016–17, the Tri-Agency supported 13 awards with a total value of $900.0M, over seven years, of which $164.8M will be distributed by CIHR to support eight awards. Over the two CFREF competitions held to date, $279.7M of the $1,249.3M awarded was distributed by CIHR to support 10 awards.
| Expected results | Performance indicators | Target | Date to achieve target | 2016–17 Actual results | 2015–16 Actual results | 2014–15 Actual results |
|---|---|---|---|---|---|---|
| CIHR-funded research contributes to a stronger health care system | Percent of CIHR priority-driven health research grants reporting contributions to strengthening the Canadian health care system | 34% | March 31, 2017 | CIHR almost met the 2016–17 target by supporting grants of which 33% reported having contributed to strengthening the Canadian health care system. This is consistent with the 2015–16 DPR result of 33%. | 33% | 35% |
| CIHR-funded research advances knowledge in emergent and specific health priorities | Percent of priority-driven health research grants reporting creation of new health knowledge | 89% | March 31, 2017 | CIHR almost met the 2016–17 target by supporting grants of which 85% reported having contributed to creating new health knowledge. This is consistent with the 2015–16 DPR result of 84%. | 84% | 88% |
| CIHR-funded research in emergent and specific health priorities results in knowledge translation | Percent of priority-driven health research grants reporting knowledge translation | 75% | March 31, 2017 | CIHR almost met the 2016–17 target by supporting grants of which 70% reported having contributed to knowledge translation. This is consistent with the 2015–16 DPR result of 72%. | 72% | 78% |
| 2016–17 Main Estimates |
2016–17 Planned spending |
2016–17 Total authorities available for use |
2016–17 Actual spending (authorities used) |
2016–17 Difference (actual minus planned) |
|---|---|---|---|---|
| 304,974,917 | 305,231,168 | 331,971,613 | 339,269,186 | 34,038,018 |
| 2016–17 Planned | 2016–17 Actual | 2016–17 Difference (actual minus planned) |
|---|---|---|
| 104 | 110 | 6 |
Information on CIHR's lower-level programs is available on the CIHR's website and in the TBS InfoBase.
Internal Services
Description
Internal Services are those groups of related activities and resources that the federal government considers to be services in support of programs and/or required to meet corporate obligations of an organization. Internal Services refers to the activities and resources of the 10 distinct service categories that support Program delivery in the organization, regardless of the Internal Services delivery model in a department. The 10 service categories are: Management and Oversight Services; Communications Services; Legal Services; Human Resources Management Services; Financial Management Services; Information Management Services; Information Technology Services; Real Property Services; Materiel Services; and Acquisition Services.
Results
CIHR continues to focus on the modernization of its existing programs, policies and information technology systems in order to better capitalize on Canada's health research strengths and address solutions to health challenges championed by Canadians.
Through its work in performance measurement and evaluation, CIHR continues to be a centre of excellence for research impact assessment in Canada and throughout the world. In 2016–17, through an internal engagement process, CIHR developed a planning, budgeting and performance information structure that meets the requirements of the new TBS Policy on Results. The structure is designed to generate departmental results that are meaningful for decision-making and government-wide reporting to Canadians. Within this evolving context, CIHR also re-aligned its resources and structure to focus and clearly define the outcomes and performance that Canadians expect from the agency. This will ensure that CIHR is positioned to implement the Policy on Results by November 2017.
In 2016–17, as part of its Equity Strategy, CIHR released its Gender Equity Framework. The Framework is designed to: (1) create an equitable funding system by identifying and eliminating systemic biases towards any individual or group that would hinder access to CIHR funds; and, (2) influence the larger health research enterprise to adopt more equitable practices.
CIHR also restructured its Institute Advisory Board (IAB) model to better align with the recommendations of the review of CIHR's slate of institutes and the Roadmap strategic plan. The members of these restructured IABs have a wide scope of scientific expertise and will identify opportunities for cross-Institute collaboration and linkages. This restructured model remains under review and will continue to be refined based on the needs of Institutes and CIHR.
CIHR launched its Strategic Action Plan on Training, designed to include a series of actions to position the next generation of researchers for success. As today's trainees will be tomorrow's peer reviewers, CIHR offered mock peer review sessions at trainee events and piloted a program to mentor outstanding postdoctoral fellows (funded through the Banting Postdoctoral Fellowships program) as reviewers of doctoral awards applications. The findings from the pilot project will help expand this program. In addition, CIHR and its partners supported the Canadian Association of Graduate Studies in a scan of professional development offerings at Canadian universities. Findings from this review will reveal existing innovations and content gaps related to sex and gender-based analysis, transferable professional skills, intersectoral experience and knowledge translation.
Guided by CIHR's Institute Evaluation Framework, in 2016–17, the Evaluation Unit completed evaluations of the Institute of Neuroscience, Mental Health and Addiction and the Institute of Musculoskeletal Health and Arthritis. Based on these evaluations, CIHR Governing Council decided to maintain the Institutes and their current mandates. Both evaluations identified the importance of Institute-specific advisory boards to support Institutes, noted challenges regarding the recruitment of the next Scientific Directors, and questioned whether Institute funding should continue to be distributed equally or scaled by burden of disease or economic cost of illness in Canada.
In addition, the CIHR Evaluation Unit, in collaboration with the Institute of Aboriginal Peoples' Health, examined CIHR's role in supporting Indigenous health research (IHR). This report informed the new Scientific Director during the Institute's transition. The report made five recommendations to enhance CIHR's role in supporting Indigenous Peoples' health research. The project informed the development of the CIHR's Action Plan: Building a healthier future for First Nations, Inuit, and Métis Peoples.
CIHR developed and began to implement a new stakeholder engagement strategy. The Strategy was designed to enhance the agency's ability to understand and identify key concerns; establish shared priorities; develop consensus and identify opportunities for collaboration: to engage key stakeholders in a meaningful and timely manner around topics of shared interest; and, to provide consistent and pro-active messaging to stakeholders. CIHR also completed consultations to bring a focus to partner engagement, explore new models for partnership and deliver greater impact for the benefit of Canadians.
| 2016–17 Main Estimates |
2016–17 Planned spending |
2016–17 Total authorities available for use |
2016–17 Actual spending (authorities used) |
2016–17 Difference (actual minus planned) |
|---|---|---|---|---|
| 28,205,865 | 28,685,620 | 30,032,008 | 31,838,217 | 3,152,597 |
| 2016–17 Planned | 2016–17 Actual | 2016–17 Difference (actual minus planned) |
|---|---|---|
| 194 | 198 | 4 |
Analysis of trends in spending and human resources
Actual expenditures
Departmental spending trend graph
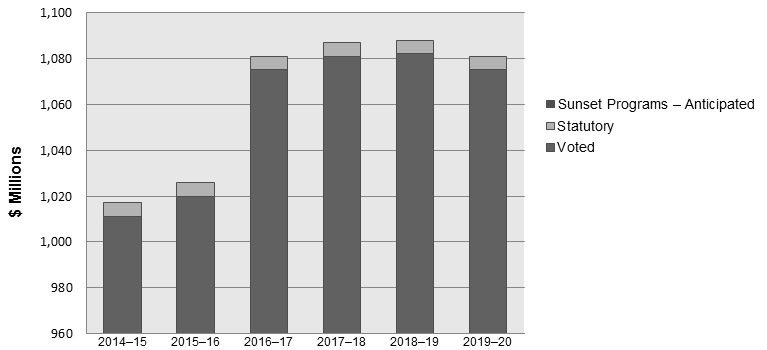
Figure 3 long description
| 2014–15 | 2015–16 | 2016–17 | 2017–18 | 2018–19 | 2019–20 | |
|---|---|---|---|---|---|---|
| Sunset Programs – Anticipated | 0 | 0 | 0 | 0 | 0 | 0 |
| Statutory | 6 | 6 | 6 | 6 | 6 | 6 |
| Voted | 1,011 | 1,020 | 1,075 | 1,081 | 1,082 | 1,075 |
| Total | 1,017 | 1,026 | 1,081 | 1,087 | 1,088 | 1,081 |
| Programs and Internal Services | 2016–17 Main Estimates |
2016–17 Planned spending |
2017–18 Planned spending |
2018–19 Planned spending |
2016–17 Total authorities available for use |
2016–17 Actual spending (authorities used) |
2015–16 Actual spending (authorities used) |
2014–15 Actual spending (authorities used) |
|---|---|---|---|---|---|---|---|---|
| 1.1 Investigator-Initiated Health Research | 692,439,221 | 692,653,215 | 729,681,747 | 736,801,477 | 721,190,915 | 710,222,941 | 692,352,816 | 703,626,155 |
| 1.2 Priority-Driven Health Research | 304,974,917 | 305,231,168 | 329,590,055 | 323,145,141 | 331,971,613 | 339,269,186 | 305,978,712 | 283,285,632 |
| Subtotal | 997,414,138 | 997,884,383 | 1,059,271,802 | 1,059,946,618 | 1,053,162,528 | 1,049,492,127 | 998,331,528 | 986,911,787 |
| Internal Services | 28,205,865 | 28,685,620 | 28,079,171 | 28,270,323 | 30,032,008 | 31,838,217 | 28,046,625 | 30,367,596 |
| Total | 1,025,620,003 | 1,026,570,003 | 1,087,350,973 | 1,088,216,941 | 1,083,194,536 | 1,081,330,344 | 1,026,378,153 | 1,017,279,383 |
CIHR's 2016–17 actual spending of $1,081.3M exceeded its planned spending of $1,026.6M by $54.7M due to the allocation of new funding. Budget 2015 allocated $15.0M new ongoing funding to CIHR, beginning in 2016–17, to expand the Strategy for Patient-Oriented Research, as well as to address antimicrobial resistance through health research. Additionally, Budget 2016 allocated $30.0M new ongoing funding to CIHR, beginning in 2016–17 to maintain and reinforce Canada's position as a leading-edge, global knowledge economy by increasing CIHR's support for early career investigators. Lastly, CIHR was allocated funding as a result of the second competition for the Canada First Research Excellence Fund (CFREF), a program that helps post-secondary institutions to excel globally in research areas that create long-term economic advantages for Canada. For this competition, CIHR received an additional $9.0M in 2016–17, and a total of $164.8M until 2022–23.
CIHR collaborates with NSERC and SSHRC on a series of Tri-Agency programs, such as the Centres of Excellence for Commercialization and Research, CFREF, the Business-Led Networks of Centres of Excellence, and the Canada Excellence Research Chairs. Funding allocated to each of the three agencies for these programs can vary between competitions depending on the recipients' alignment with the research mandate and priorities of each agency. Accordingly, funding allocations are confirmed and included in planned spending once the competition results are available. As such, CIHR's planned spending is expected to increase as a result of successful health-oriented projects within future competitions.
CIHR also collaborates on partnership activities with other federal departments and agencies and, as a result, funding may be transferred to CIHR to address a common theme or research priority. As partnership activities are confirmed in the upcoming fiscal years, it is anticipated that CIHR's planned spending will increase.
The actual spending for 2014–15 and 2015–16 by Programs and Internal Services was realigned to reflect a change in methodology used by CIHR to record and report its internal services following the implementation of the Treasury Board of Canada Secretariat Guide on Recording and Reporting of Internal Services Expenditures. As a result, operational funding and FTEs for some of CIHR's supporting units are now recorded as Internal Services, whereas they were previously reported within CIHR's Investigator-Initiated or Priority-Driven Programs.
The increase of $3.8M in Internal Services over 2015–16 actual spending and 2016–17 planned spending was due to greater salary expenditures, as a result of a greater number of FTEs, increased professional and special services expenditures, and increased purchases of furniture, equipment and software during the 2016–17 fiscal year.
Actual human resources
| Programs and Internal Services | 2014–15 Actual |
2015–16 Actual |
2016–17 Planned |
2016–17 Actual |
2017–18 Planned |
2018–19 Planned |
|---|---|---|---|---|---|---|
| 1.1 Investigator-Initiated Health Research | 109 | 105 | 104 | 117 | 125 | 120 |
| 1.2 Priority-Driven Health Research | 108 | 104 | 104 | 110 | 122 | 123 |
| Subtotal | 217 | 209 | 208 | 227 | 247 | 243 |
| Internal Services | 202 | 194 | 194 | 198 | 209 | 209 |
| Total | 419 | 403 | 402 | 425 | 456 | 452 |
In 2015–16, CIHR completed an internal reorganization, which resulted in the realignment of resources and a number of positions remaining vacant until the reorganization was fully implemented. This reorganization also resulted in the temporary freezing of positions in 2015–16 and forecasted to remain frozen in 2016–17.
In 2016–17, CIHR unfroze all vacant positions due to operational requirements, and created positions to deliver the programs and initiatives funded from both Budget 2015 and Budget 2016, as well as positions to implement the recommendations stemming from the Working Meeting to discuss CIHR peer review processes with the research community.
As positions were unfrozen or created in 2016–17, CIHR staffed some positions in the latter part of the fiscal year, and anticipates these positions to be fully staffed in 2017–18.
Expenditures by vote
For information on the Canadian Institutes of Health Research's organizational voted and statutory expenditures, consult the Public Accounts of Canada 2017.
Alignment of spending with the whole-of-government framework
| Program | Spending area | Government of Canada activity | 2016–17 Actual spending |
|---|---|---|---|
| 1.1 Investigator-Initiated Health Research | Social Affairs | Healthy Canadians | 710,222,941 |
| 1.2 Priority-Driven Health Research | Social Affairs | Healthy Canadians | 339,269,186 |
| Spending area | Total planned spending | Total actual spending |
|---|---|---|
| Economic affairs | 0 | 0 |
| Social affairs | 997,884,383 | 1,049,492,127 |
| International affairs | 0 | 0 |
| Government affairs | 0 | 0 |
Financial statements and financial statements highlights
Financial statements
The CIHR's financial statements (unaudited) for the year ended March 31, 2017, are available on the CIHR's website.
Financial statements highlights
| Financial information | 2016–17 Planned resultsFootnote * |
2016–17 Actual |
2015–16 Actual |
Difference (2016–17 actual minus 2016–17 planned) |
Difference (2016–17 actual minus 2015–16 actual) |
|---|---|---|---|---|---|
| Total expenses | 1,038,365,000 | 1,088,137,000 | 1,036,152,000 | 49,772,000 | 51,985,000 |
| Total revenues | 10,075,000 | 6,864,000 | 7,806,000 | (3,211,000) | (942,000) |
| Net cost of operations before government funding and transfers | 1,028,290,000 | 1,081,273,000 | 1,028,346,000 | 52,983,000 | 52,927,000 |
CIHR's actual total expenses were approximately $49.8M higher than planned, due primarily to investment resulting from Budget 2015 and Budget 2016 and the second competition for the CFREF program, approved via the Supplementary Estimates (which were unknown at the time that 2016–17 planned results were determined). Refer to the Budgetary performance summary for Programs and Internal Services for further details. Total revenues fluctuate annually as they depend exclusively on the timing of receiving partner funding and disbursing that partner funding to health researchers. CIHR received fewer partner donations in 2016–17.
In 2016–17, CIHR determined that expenses related to two internally developed software assets were not capitalized over the past two fiscal years. As a result of the error, assets were understated and expenses were overstated in fiscal 2014–15 and 2015–16. The changes have been applied retroactively and the prior year balances have been adjusted accordingly. As such, expenses for the year ended March 31, 2016 were decreased by $1.9M less $0.2M in amortization expense.
CIHR's higher than planned total expenses of $49.8M in 2016–17 and lower than planned total revenues of approximately $3.2M resulted in the net cost of operations before government funding and transfers being approximately $53.0M higher than planned for the fiscal year.
| Financial information | 2016–17 | 2015–16 | Difference (2016–17 minus 2015–16) |
|---|---|---|---|
| Total net liabilities | 13,563,000 | 14,049,000 | (486,000) |
| Total net financial assets | 12,636,000 | 11,045,000 | 1,591,000 |
| Departmental net debt | 927,000 | 3,004,000 | (2,077,000) |
| Total non-financial assets | 7,046,000 | 4,979,000 | 2,067,000 |
| Departmental net financial position | 6,119,000 | 1,975,000 | 4,144,000 |
The slight decrease of $0.5M in total liabilities is primarily due to a decrease in deferred revenue as a result of lower external partner donations for research. The decrease was offset by an increase to accounts payable and accrued liabilities due to an additional day of accrued payroll and due to the timing of invoice payments.
The increase in total financial and non-financial assets of $3.7M is primarily due to a $2.0M increase in tangible capital assets as a result of the capitalization of various internally developed software. Additionally, there was a $1.8M increase in accounts receivable and advances mainly due to grant refunds owing at year-end.
As mentioned above, in 2016–17, CIHR determined that expenses related to two internally developed software assets were not capitalized over the past two fiscal years. The changes to correct the error have been applied retroactively and tangible capital assets as at March 31, 2016 were increased by $4.2M and the opening Departmental net financial position as of April 1, 2015 was increased by $2.5M.
Supplementary information
Corporate information
Organizational profile
Appropriate minister: The Honourable Ginette Petitpas Taylor, P.C., M.P.
Institutional head: Dr. Roderick McInnes, President (Acting President)
Ministerial portfolio: Health
Enabling instrument: Canadian Institutes of Health Research Act (S.C. 2000, c. 6)
Year of incorporation / commencement: 2000
Reporting framework
The Canadian Institutes of Health Research Strategic Outcome and Program Alignment Architecture (PAA) of record for 2016–17 are shown below:
- 1. Strategic Outcome: Canada is a world leader in the creation, dissemination and application of health research knowledge
- 1.1 Program: Investigator-Initiated Health Research
- 1.1.1 Sub-Program: Operating Support
- 1.1.2 Sub-Program: Training and Career Support
- 1.2 Program: Priority-Driven Health Research
- 1.2.1 Sub-Program: Institute-Driven Initiatives
- 1.2.2 Sub-Program: Horizontal Health Research Initiatives
- Internal Services
- 1.1 Program: Investigator-Initiated Health Research
Supporting information on lower-level programs
Supporting information on results, financial and human resources relating to the CIHR lower-level programs is available on InfoBase.
Supplementary information tables
The following supplementary information tables are available on the CIHR's website:
- Departmental Sustainable Development Strategy
- Details on transfer payment programs of $5 million or more
- Internal audits and evaluations
Federal tax expenditures
The tax system can be used to achieve public policy objectives through the application of special measures such as low tax rates, exemptions, deductions, deferrals and credits. The Department of Finance Canada publishes cost estimates and projections for these measures each year in the Report on Federal Tax Expenditures. This report also provides detailed background information on tax expenditures, including descriptions, objectives, historical information and references to related federal spending programs. The tax measures presented in this report are the responsibility of the Minister of Finance.
Organizational contact information
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
Canada
Appendix: definitions
- appropriation (crédit)
- Any authority of Parliament to pay money out of the Consolidated Revenue Fund.
- budgetary expenditures (dépenses budgétaires)
- Operating and capital expenditures; transfer payments to other levels of government, organizations or individuals; and payments to Crown corporations.
- Core Responsibility (responsabilité essentielle)
- An enduring function or role performed by a department. The intentions of the department with respect to a Core Responsibility are reflected in one or more related Departmental Results that the department seeks to contribute to or influence.
- Departmental Plan (Plan ministériel)
- Provides information on the plans and expected performance of appropriated departments over a three-year period. Departmental Plans are tabled in Parliament each spring.
- Departmental Result (résultat ministériel)
- A Departmental Result represents the change or changes that the department seeks to influence. A Departmental Result is often outside departments' immediate control, but it should be influenced by program-level outcomes.
- Departmental Result Indicator (indicateur de résultat ministériel)
- A factor or variable that provides a valid and reliable means to measure or describe progress on a Departmental Result.
- Departmental Results Framework (cadre ministériel des résultats)
- Consists of the department's Core Responsibilities, Departmental Results and Departmental Result Indicators.
- Departmental Results Report (Rapport sur les résultats ministériels)
- Provides information on the actual accomplishments against the plans, priorities and expected results set out in the corresponding Departmental Plan.
- Evaluation (évaluation)
- In the Government of Canada, the systematic and neutral collection and analysis of evidence to judge merit, worth or value. Evaluation informs decision making, improvements, innovation and accountability. Evaluations typically focus on programs, policies and priorities and examine questions related to relevance, effectiveness and efficiency. Depending on user needs, however, evaluations can also examine other units, themes and issues, including alternatives to existing interventions. Evaluations generally employ social science research methods.
- full-time equivalent (équivalent temps plein)
- A measure of the extent to which an employee represents a full person-year charge against a departmental budget. Full-time equivalents are calculated as a ratio of assigned hours of work to scheduled hours of work. Scheduled hours of work are set out in collective agreements.
- government-wide priorities (priorités pangouvernementales)
- For the purpose of the 2017–18 Departmental Plan, government-wide priorities refers to those high-level themes outlining the government's agenda in the 2015 Speech from the Throne, namely: Growth for the Middle Class; Open and Transparent Government; A Clean Environment and a Strong Economy; Diversity is Canada's Strength; and Security and Opportunity.
- horizontal initiatives (initiative horizontale)
- An initiative where two or more federal organizations, through an approved funding agreement, work toward achieving clearly defined shared outcomes, and which has been designated (for example, by Cabinet or a central agency) as a horizontal initiative for managing and reporting purposes.
- Management, Resources and Results Structure (Structure de la gestion, des ressources et des résultats)
- A comprehensive framework that consists of an organization's inventory of programs, resources, results, performance indicators and governance information. Programs and results are depicted in their hierarchical relationship to each other and to the Strategic Outcome(s) to which they contribute. The Management, Resources and Results Structure is developed from the Program Alignment Architecture.
- non-budgetary expenditures (dépenses non budgétaires)
- Net outlays and receipts related to loans, investments and advances, which change the composition of the financial assets of the Government of Canada.
- performance (rendement)
- What an organization did with its resources to achieve its results, how well those results compare to what the organization intended to achieve, and how well lessons learned have been identified.
- performance indicator (indicateur de rendement)
- A qualitative or quantitative means of measuring an output or outcome, with the intention of gauging the performance of an organization, program, policy or initiative respecting expected results.
- performance reporting (production de rapports sur le rendement)
- The process of communicating evidence-based performance information. Performance reporting supports decision making, accountability and transparency.
- planned spending (dépenses prévues)
- For Departmental Plans and Departmental Results Reports, planned spending refers to those amounts that receive Treasury Board approval by February 1. Therefore, planned spending may include amounts incremental to planned expenditures presented in the Main Estimates.
- A department is expected to be aware of the authorities that it has sought and received. The determination of planned spending is a departmental responsibility, and departments must be able to defend the expenditure and accrual numbers presented in their Departmental Plans and Departmental Results Reports.
- plans (plans)
- The articulation of strategic choices, which provides information on how an organization intends to achieve its priorities and associated results. Generally a plan will explain the logic behind the strategies chosen and tend to focus on actions that lead up to the expected result.
- priorities (priorité)
- Plans or projects that an organization has chosen to focus and report on during the planning period. Priorities represent the things that are most important or what must be done first to support the achievement of the desired Strategic Outcome(s).
- program (programme)
- A group of related resource inputs and activities that are managed to meet specific needs and to achieve intended results and that are treated as a budgetary unit.
- Program Alignment Architecture (architecture d'alignement des programmes)
- A structured inventory of an organization's programs depicting the hierarchical relationship between programs and the Strategic Outcome(s) to which they contribute.
- results (résultat)
- An external consequence attributed, in part, to an organization, policy, program or initiative. Results are not within the control of a single organization, policy, program or initiative; instead they are within the area of the organization's influence.
- statutory expenditures (dépenses législatives)
- Expenditures that Parliament has approved through legislation other than appropriation acts. The legislation sets out the purpose of the expenditures and the terms and conditions under which they may be made.
- Strategic Outcome (résultat stratégique)
- A long-term and enduring benefit to Canadians that is linked to the organization's mandate, vision and core functions.
- sunset program (programme temporisé)
- A time-limited program that does not have an ongoing funding and policy authority. When the program is set to expire, a decision must be made whether to continue the program. In the case of a renewal, the decision specifies the scope, funding level and duration.
- target (cible)
- A measurable performance or success level that an organization, program or initiative plans to achieve within a specified time period. Targets can be either quantitative or qualitative.
- voted expenditures (dépenses votées)
- Expenditures that Parliament approves annually through an Appropriation Act. The Vote wording becomes the governing conditions under which these expenditures may be made.
- Date modified: