Review of the Institute of Gender and Health
Report of the IGH Review Panel
June 2018
At the Canadian Institutes of Health Research (CIHR), we know that research has the power to change lives. As Canada's health research investment agency, we collaborate with partners and researchers to support the discoveries and innovations that improve our health and strengthen our health care system.
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
This publication was produced by the Canadian Institutes of Health Research. The views expressed herein do not necessarily reflect those of the Canadian Institutes of Health Research.
IGH Review Panel:
Chair: Gillian Einstein, Wilfred and Joyce Posluns Chair of Women's Brain Health and Aging; Associate Professor, Department of Psychology, University of Toronto; Adjunct Scientist, Women's College Research Institute; Founder, Collaborative Graduate Program in Women's Health, University of Toronto
Panel Members:
- Geert de Vries, Professor, Neuroscience Institute and Associate Vice President for Research & Economic Development, Georgia State University
- Sylvie Mader, Principal Investigator, Molecular Targeting in Breast Cancer Research Unit, IRIC; Professor, Department of Biochemistry, Faculty of Medicine, Université de Montréal
- Cindy Moriarty, Executive Director, Health Programs and Strategic Initiatives, Strategic Policy Branch, Health Canada
- John Oliffe, Professor and Associate Director of Research, School of Nursing, University of British Columbia; Founder and Lead Investigator, University of British Columbia's Men's Health Research program
- Londa Schiebinger, John L. Hinds Professor, History of Science, Stanford University; Director, EU/US Gendered Innovations in Science, Health & Medicine, Engineering and Environment Project
Thanks to all participants in this review and the CIHR IGH Review Team: Ian Raskin, Michael Goodyer, Carmelle Goldberg, Kim Gaudreau, Christopher Manuel, Jonathan Gilbert, and Carole Chow.
And special thanks to:
- Dr. Cara Tannenbaum, Scientific Director, IGH
- Krystle van Hoof, Assistant Director, IGH, and the IGH team
For more information and to obtain copies, please contact: Evaluation@cihr-irsc.gc.ca.
Table of Contents
- Executive Summary
- Overview of the Review and IGH
- Observations and Recommendations
- Key Findings
- References
- Appendices
I. Executive Summary
The review of the Institute of Gender and Health (IGH) was undertaken by the Canadian Institutes of Health Research (CIHR) as part of the review of the mandate and performance of CIHR Institutes by CIHR’s Governing Council (GC) outlined in the CIHR Act. The review assessed the relevance and performance of IGH to inform decisions regarding the role and functioning of the Institute. The review was conducted by the CIHR Evaluation Unit and overseen by the IGH Review Panel (hereafter referred to as the Panel)—a panel of experts in IGH’s mandate areas who reviewed and interpreted the findings and made the final recommendations. The observations and recommendations of the Panel are summarized below in relation to the three broad issues addressed by the review.
Are changes needed within the current IGH mandate in order to address emerging areas of research?
The Panel concluded that IGH’s mandate is appropriate. It is broad enough to continue facilitating the growth of IGH activities as well as the growth of the field of sex and gender science. The Panel commended IGH’s progress in: 1) advancing the field of sex and gender science (Innovation); 2) Integrating sex and gender in health research, programs and policies (Integration); and 3) translating descriptive sex and gender health research to interventions that improve health outcomes (Impact). However, given the breadth and more pressing nature of the workload associated within fulfilling IGH’s mandate, the Panel recommended additional resources and/or support for IGH from CIHR. Given the current political imperative to implement CIHR’s Sex- and Gender-Based Analysis (SGBA) Action Plan and IGH’s important leadership role in this, the Panel recommended quick action in this regard to take full advantage of this opportunity and to sustain and scale IGH’s current momentum.
Recommendation 1: The Panel recommends that IGH continue to fulfill the roles stated in its current mandate.
Recommendation 2: The Panel recommends that IGH continue to play a strategic leadership role, domestically and internationally, in fostering and strengthening sex and gender science. Specific areas for action include scaling partnerships with academic institutions, policy-makers, funders and the research community to increase the reach and visibility of IGH’s leadership, work and funded research.
Recommendation 3: The Panel recommends that CIHR, in collaboration with IGH, review how CIHR is fulfilling its SGBA commitments and, specifically, to what extent CIHR relies on IGH to meet these commitments. Unlike other CIHR Institutes, IGH is called upon to support CIHR’s implementation of the Government of Canada’s Health Portfolio SGBA Policy.Footnote 1 While the Panel supported the need to leverage IGH’s expertise, this work needs to be adequately resourced and should not come from IGH’s existing annual budget.
Recommendation 4: The Panel recommends that CIHR re-assess the resources allocated to IGH and specifically consider the following:
- Increase the current Scientific Director (SD) from 0.50 to 0.75 of a full time equivalentFootnote 2 (FTE);
- Increase IGH’s annual budget allocation as a proportion of the $354.7M increase allocated to CIHR in Budget 2018 to build capacity to advance the field of sex and gender science; and,
- Increase the staff complement to ensure adequate support to the SD and IGH to fulfill its mandate and roles. This should include: re-instating the one FTE at the Assistant Director level based in Ottawa to integrate the roles of IGH and CIHR in relation to SGBA, ensuring any existing vacancies are filled at IGH, and considering the need for additional IGH staff at the host institution to scale and assess integration and knowledge translation activities.
Recommendation 5: The Panel recommends the name of the Institute be changed to the Institute of Gender, Sex and Health to more fully reflect its mandate to national and international research and stakeholder communities.
Should the IGH Scientific Director be renewed?
Recommendation 6: The Panel strongly recommends that the current IGH Scientific Director be renewed. Dr. Tannenbaum’s exceptional achievements in her first term affirm her as uniquely suited to deliver on IGH’s 2018–23 strategic plan.
Other Observations, Considerations or Recommendations
The Panel supports the renewal of IGH’s strategic plan to refresh its ten goals and outline key actions and indicators that build on the work and achievements of the 2013–17 strategic plan (Strategy 2017). The 2018–23 strategic plan is a relevant and important next step that should be implemented in consultation with the IGH’s incoming IAB. The Panel strongly encourages the SD to further strategiaclly appoint and harness the energy of all IGH Institute Advisory Board (IAB) members to further advance the reach and impact of the institute.
Recommendation 7: The Panel recommends that IGH’s strategic plan for 2018–23 be launched.
Recommendation 8: The Panel recommends that IGH be provided the resources necessary to monitor the impacts of their special calls as well as CIHR funded research under the IGH mandate. Specifically, end of grant reports for grants intending to include sex and/or gender considerations should be reviewed to formally assess the investments made toward sex and gender research. In addition, bibliometrics should be collected independently of these report data to provide a baseline from which to measure publication impact and output.
II. Overview of the Review and IGH
A. Review Objectives
The review of the Institute of Gender and Health (IGH) was conducted by the Canadian Institutes for Health Research (CIHR) as part of the rolling review of the mandate and performance of the 13 CIHR Institutes as mandated by the CIHR Act and the Policy on Results.
The IGH review aims to support CIHR to address the following questions:
- Are changes needed within the current IGH mandate to address emerging areas of research?
- Should the IGH Scientific Director be renewed?
The review was overseen by the IGH Review Panel comprising experts in the IGH mandate areas who reviewed and interpreted the findings and made the final recommendations. The names and affiliations of the Panel members are listed in Appendix 1. The review was conducted by the CIHR Evaluation Unit.
Because the formation of IGH has been an integral development in the new and growing field of sex and gender science, the review covered the period 2000–17. However, it focused on the period 2015–18 to assess the leadership of the current SD, Dr. Cara Tannenbaum. The review framework drew on multiple lines of evidence, including qualitative and quantitative data sources outlined in Appendix 2 with key figures presented in Appendix 3. The review used administrative data on expenditures related to the IGH mandate, bibliometric analysis on the ranking of Canada compared to the top active countries in four priority areas defined by IGH, interviews with IGH researchers and stakeholder representatives and Panel deliberations. While each line of evidence has limitations, multiple data sources were triangulated to produce key findings. Overall, the Panel is confident that the key findings presented in this report provide an accurate account of the relevance of IGH’s mandate and its performance based on information available and the indicators addressed.
B. IGH Context
As one of the 13 CIHR Institutes, IGH has a scientific vision of a world where sex and gender are integrated as key considerations across health research and translated into personalized and population health in a real-world setting. Congruent with this mandate, IGH funds work to address sex differences and health disparities falling along sex and gender lines as well as working to foster the inclusion of sex and gender considerations in all research. The role of IGH is to support and champion a health research agenda that embraces consideration of sex and gender in a manner that is both scientifically rigorous and responsive to the diverse health needs of people in Canada and around the world. The mission is to foster research excellence regarding the influence of sex and gender on health and to apply these findings to identify and address pressing health challenges facing men, women, girls, boys and gender-diverse people.Footnote 3
As outlined in IGH’s 2018–23 strategic plan, IGH’s approach to innovation seeks to support leading sex and gender researchers to question assumptions, integrate gender-transformative approaches and investigate the causal mechanisms underlying sex and gender differences. Further, to fulfill the impact strategic direction in the new strategic plan, IGH will build relationships across the health ecosystem to translate sex and gender science into personalized health at the point of care.
In addition to this, IGH is leading the development of the new field of sex and gender science. Much like the development of the field of neuroscience, sex and gender science is emerging from individual research disciplines by incorporating consideration of sex and gender into existing experimental approaches as well as developing methods designed specifically to ask questions about how sex and gender influence the etiology, progress, and treatment of diseases in men, women, boys, girls, and gender-diverse people. The manifestation of this new expertise is beginning to be seen in the development of “Sex and Gender Champions”—researchers who promote the integration of sex and gender across multiple health and illness issues. Thus, IGH’s leadership has begun to build a new field of sex (biological factors) and gender (socio-cultural factors) science.
III. Observations and Recommendations
A. Are changes needed within the current IGH mandate to address emerging areas of research?
Context
The IGH mandate supports health research that takes sex and gender into account, making it responsive to the health needs of men, women, boys, girls, and gender-diverse people in Canada and around the world. To fulfill its mission, IGH plays an important leadership role in advancing knowledge, building capacity in sex, gender and health research across disciplines and career stages, and accelerating the application of evidence in the real world. Working with modest funding, IGH has consulted with the community extensively to focus its efforts on the strategic priorities of Integration, Innovation, and Impact. These three strategic directions are supported by ten goals, geared towards transformation that extends from funding opportunities in “priority” topic areas to how IGH can shape science more broadly through the creation and application of new knowledge.
In line with IGH’s mandate, in 2010–11, CIHR introduced a mandatory requirement for all CIHR grant applicants to indicate how their research incorporates sex and/or gender considerations. These processes both encouraged investigators to bring considerations of sex and gender into their research as well as flag their applications as intending to incorporate sex and/or gender. Thus, the number of applications considering sex and gender has increased the number of grants classified under the IGH mandate, resulting in a significant increase in the amount of CIHR investment attributed to the IGH mandate (see Figure A in Appendix 3).
CIHR investments in IGH’s strategic directions can be divided into investments that go toward IGH’s strategic direction of Integration and those that go into IGH’s strategic direction of Innovation. Funded research that incorporates sex and/or gender, but does not align with the Institutes’ mandate, is classified as investment in Integration; funded research attributed to the Institute’s mandate through keyword validation is classified as investment in Innovation.
CIHR investment in Integration rose from $3M to $212M (from 58 funded applications to 1762) from 2011–12 to 2015–16, decreasing to $193M (1125 funded applications) from 2015–16 to 2016–17. Simultaneously, CIHR investments classified as Innovation increased from $86M (1122 funded applications) in 2011–12 to $178M (1572 funded applications) in 2015–16, peaking at $288M (2448 funded applications) in 2016–17 (see Figure A in Appendix 3). The increase in CIHR’s investments in IGH’s mandate in the area of Integration is likely an overestimate as compliance has not been assessed by CIHR. However, the increase in the area of Innovation can be viewed as contributing to the development of the field of sex and gender science.
IGH’s mandate is directly aligned with the Government of Canada’s Health Portfolio Sex- and Gender-Based Analysis (SGBA) Policy and the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans. Because of this mandate, IGH has also taken a leadership role in building capacity within government organizations to develop SGBA action plans integrating the effects of sex and gender into services, programs, and policy.
Panel Observations and Recommendations
The Panel unanimously agreed that IGH exceeded expectations as the world’s first and only research funding institute with a specific focus on sex, gender and health. The Panel noted the successes and achievements in building awareness of the importance of sex and gender considerations and changing behaviours of diverse national and international stakeholders. In particular, the Panel commends IGH’s leadership and partnerships across CIHR in multi-institute initiatives, as well as internationally through partnerships with the European Union, the Office for Research on Women’s Health (US), the Matera Alliance,Footnote 4 and ZonMW.Footnote 5 Specifically, Canada’s international visibility and leadership in the sex and gender field has been, and will continue to be, catalyzed by IGH’s continued brokering of high impact international partnerships and collaborations such as GENDER-NET Plus and the Matera Alliance. Further, the development and implementation of core competency e-learning modules for researchers, peer reviewers, and trainees was said to build competence within Canada. IGH’s development of Sex and Gender Champions is also playing a role in developing sex and gender science. The Panel noted the significant advances in women’s, and boys’ and men’s health, the impact of gender-sensitized knowledge translation interventions, and inclusion of sex as a variable in biomedical research that have emerged from IGH investments.
Many foundational discoveries have revealed that sex and gender matter across all pillars of health research: from the biology of the cell to their impact on society. The past ten years have seen promising developments pertaining to sex and gender in the scientific landscape, which have been supported by CIHR as well as other organizations. The Panel observed that IGH’s strategic directions to foster the integration of sex and gender in health research (Integration), and promote scientific discoveries in sex and gender health research (Innovation) is crucial to the development of the field of sex and gender science. The Panel concluded that IGH’s mandate should not be changed as it is critical to the development and advancement of this new field both in Canada and internationally.
Recommendation 1: The Panel recommends that IGH continue to fulfill the roles stated in its current mandate.
Further, the Panel encouraged IGH to focus its current resources on building the field of sex and gender science as well as accelerating discoveries in sex and gender health research through novel approaches, and methods and measures. The Panel unanimously agreed that investments in new cell/animal models and research approaches as well as applications will continue to move the field of sex and gender science forward. An emerging priority is to translate these new methods and methodologies into updated guidelines and manuals for diverse stakeholders. These investments will allow IGH to maintain its leadership role, and push this new field of sex and gender science forward both in Canada and internationally.
The Panel concluded that IGH’s mandate is appropriate and broad enough to meet increasing developments in the field. However, this places demands on IGH’s resources to respond to increasing needs in each of its three strategic directions. First, IGH’s role in the Integration of sex and gender into other areas of health research is expanding beyond CIHR’s budget allocation to IGH and also beyond research to CIHR and other federal government programs and policies. In the area of Innovation, IGH has a unique and pressing responsibility to advance and disseminate sex and gender health research and continue to build and lead the field of sex and gender science both nationally and internationally. The demand to the strategic direction, Impact, can be expected to increase in both policy and practice, given IGH’s achievements in Integration through their work with government departments to ensure policies are responsive to sex and gender considerations. There will also be an increased demand to the strategic direction of Innovation in order to grow knowledge translation capacity to support the dissemination and application of research findings to sex- and gender-specific health-care practices.
Recommendation 2: The Panel recommends that IGH continue to play a strategic leadership role, domestically and internationally, in fostering and strengthening sex and gender science. Specific areas for action include scaling partnerships with academic institutions, policy-makers, funders and the research community to increase the reach and visibility of IGH’s leadership, work and funded research.
The Panel commended IGH’s expertise in the Integration of sex and gender considerations within and across health research funding at CIHR, with funders and research ethics boards. A key component of IGH’s Integration activities have been the provision of its expertise and resources to the leadership and implementation of CIHR’s SGBA Action Plan as well as leadership and advice on SGBA application within the federal government.
Recognizing that IGH holds vital expertise in SGBA, it is important that IGH continue to support CIHR in the implementation of the SGBA Action Plan as part of the Government of Canada’s commitment to SGBA requiring that sex and gender be fully considered and systematically incorporated into policy, programs, and services. Given the political imperative to implement CIHR’s SGBA Action Plan and IGH’s important leadership role in its implementation, the Panel identified the need for IGH to be involved in ensuring the SGBA mandate is met and additional resources should be directed to IGH in order to fulfill these responsibilities without taking limited resources away from other responsibilities under its mandate.
Recommendation 3: The Panel recommends that CIHR, in collaboration with IGH, review how CIHR is fulfilling its SGBA commitments and, specifically, to what extent CIHR relies on IGH to meet these commitments. Unlike other CIHR Institutes, IGH is called upon to support CIHR’s implementation of the Government of Canada’s Health Portfolio SGBA.Footnote 6 While the Panel supported the need to leverage IGH’s expertise, this work needs to be adequately resourced and should not come from IGH’s existing annual budget.
The Panel observed numerous demands on IGH within its mandate in terms of its stated role to: 1) advance and disseminate sex and gender science (Innovation) as well as continue to lead the field; 2) integrate sex and gender in science as well as programs and policies, including CIHR’s SGBA Action Plan; and 3) translate sex and gender health research findings to improve health outcomes. Given the breadth and increasing nature of these needs within IGH’s mandate and current resources available, the Panel is concerned that it will be very difficult to meet these needs and, by extension, its mandate, without additional resources and/or support from CIHR. The Panel noted three areas where resources are expected to be needed to meet these increased needs within IGH’s mandate:
- The time available to the SD to provide expertise, engage researchers, stakeholders and knowledge users, and fulfil the role of SGBA Champion may not be feasible under the current arrangement of time dedicated to the role of CIHR Scientific Director—expected to be 50% of working hours;
- Resources to support Institute operations in light of the loss of Ottawa-based Institute staff (OBIS) dedicated to IGH and corporate knowledge in the move to the matrix model of Integrated Institute Teams (IIT) as well as the need for additional staff to effectively deliver on the strategic directions; and,
- Funding for IGH specific research initiatives to continue to lead and advance the field of sex and gender science by funding innovative and excellent research, enhance the capacity of the research community, and ensure its translation to and application in both policy and practice.
In addition, there is a fourth need within IGH’s mandate which is not simply advancing an already established field but leading the development of an emerging field of ‘Sex and Gender Science’. An analysis of IGH mandate investment data show that investments in Innovation exceeded those of Integration, suggesting a successful transition from researchers merely including sex and gender as variables in their study designs towards more thorough considerations, which have the potential to translate into Innovations in the field of sex and gender science.
In summary, it is important to note that, within its mandate, IGH now does the following:
- Supports the advancement and application of sex and gender in health research;
- Supports CIHR in its new role and overall commitment to applying sex and gender across the organization (SBGA)—an expanded role within its mandate;
- Translates sex and gender health research findings to improve health outcomes; and,
- Nurtures and develops the new field of sex and gender science, which is a new and developing role within the mandate since the 2013–17 strategic plan.
Recommendation 4: The Panel recommends that CIHR re-assess the resources allocated to IGH and specifically consider the following:
- Increase the current Scientific Director (SD) from 0.50 to 0.75 of a full time equivalentFootnote 7 (FTE);
- Increase IGH’s annual budget allocation as a proportion of the $354.7M increase allocated to CIHR in Budget 2018 to build capacity to advance the field of sex and gender science; and,
- Increase the staff complement to ensure adequate support to the SD and IGH to fulfill its mandate and roles. This should include: re-instating the one FTE at the Assistant Director level based in Ottawa to integrate the roles of IGH and CIHR in relation to SGBA, ensuring any existing vacancies are filled at IGH, and considering the need for additional IGH staff at the host institution to scale and assess integration and knowledge translation activities.
Finally, the Panel identified a need to change IGH’s name to the Institute of Gender, Sex, and Health to more fully reflect the state of the science and to explicitly communicate its mandate to researcher and stakeholder communities nationally and internationally. The Panel debated as to whether sex or gender should be the first term in the new name but consensus was to put gender first to link the new name clearly with the original name.
Recommendation 5: The Panel recommends the name of the Institute be changed to the Institute of Gender, Sex and Health to more fully reflect its mandate to national and international research and stakeholder communities.
B. Should the IGH Scientific Director be renewed?
Context
The current SD, Dr. Cara Tannenbaum, started her term in January 2015, inheriting the 2013–17 strategic plan of the preceding SD in the early days of its implementation. The current SD worked on operationalizing the 2013–17 strategic plan, and, in 2017, renewed and advanced IGH’s commitment to the strategic directions of Integration, Innovation and Impact. She aims to further shape and accelerate the integration of sex as a biological variable and gender as a socio-cultural determinant of health to advance sex and gender knowledge across the four CIHR pillars. IGH’s latest strategic plan (2018–23) is currently pending approval by CIHR.
During the first term of the SD, several changes implemented at CIHR impacted the allocation of resources to all the institutes. First, the Roadmap Accelerator Fund (RAF) required the Institutes to reallocate half their budgets to the RAF. Second, the Institute Advisory Boards (IAB) for each Institute were ended in July 2016 and a new model of five cross-cutting thematic IABs aligned with the strategic directions and research priorities of CIHR’s five-year strategic plan, Health Research Roadmap II, was instituted. In 2017–18, the model of one IAB per institute was re-instated and is currently being implemented. Third, the Ottawa-based Institute staff (OBIS), who were dedicated Ottawa-based personnel providing service to one Institute, were reformed into Institute Teams (IIT), serving all of the Institutes. The Panel observed that these three reorganizations were particularly difficult for a new SD—especially one with such a broad stakeholder community, a huge dissemination and teaching responsibility, and a nascent field to develop. The Panel commended the SD for not only managing well under these circumstances but flourishing and developing the field of sex and gender science.
Panel Observations and Recommendations
IGH has benefitted from strong leadership since its inception and the Panel commended the leadership provided by the current SD during a challenging period of transition at CIHR. The SD has considerable strengths reflected in moving sex and gender considerations towards broad implementation, accountability and impact. The SD is a leading source of information in the field, as well an active spokesperson, mentor, and advocate for SGBA in health research. Her academic, research, and clinical perspectives were consistently highlighted as important strengths by key informants, allowing Dr. Tannenbaum to interface well within all sectors and with diverse stakeholders. The SD also clearly contributes as an effective member of the CIHR management team and collaborator with other Institutes and the broader research community nationally and internationally.
The Panel found that under the leadership of the current SD, the Institute has identified and leveraged strategic research investments with other government agencies and the private sector in high impact areas. Some examples include: the Policy-Research Partnerships, the Healthy and Productive Work Initiative, the Matera Alliance, and GENDER-NET Plus. The Panel further notes that the SD is actively addressing partnership challenges with other government agencies and the not-for-profit sector and recommends that increased resources, flexibility and autonomy would enable Dr. Tannenbaum to more fully engage a range of partners and diverse stakeholders.
The Panel also found that under the leadership of Dr. Tannenbaum, a new field, sex and gender science, has been emerging in Canada and internationally, led to a great degree by IGH. Specifically, when compared to other fields, sex and gender science is in its early days. However, many foundational discoveries have revealed that sex and gender matter across all pillars of research: from the cell to society. Footnote 8,Footnote 9
Given Dr. Tannenbaum’s exceptional achievements in her first term, and fact that IGH is poised to deliver on a renewed strategic plan, the Panel felt that continuity of leadership is very important at this time to solidify and further build the field of sex and gender science. The SD has a strong vision and excellent follow-through on her goals, but requires additional supports and resources to effectively execute IGH’s vision and keep it in the lead internationally. IGH is continually looked to for leadership in sex and gender research and it is acknowledged internationally that Canada has a unique perspective that strives to include both sex and gender rather than just one or the other. The Panel encouraged the SD to reflect on how to strategically appoint and harness the collective energy of the soon to be appointed IAB members and the Sex and Gender Champions to advance the reach and impact of the Institute.
Recommendation 6: The Panel strongly recommends that the current IGH Scientific Director be renewed.
C. Other Observations and Recommendations
Panel Observations and Recommendations
As part of the review, the Panel reviewed IGH’s strategic plan for 2018–23. The Panel noted IGH’s extensive community outreach to build consensus in the research community in the preparation of the next strategic plan. The strategic plan renews and advances IGH’s commitment to the strategic directions of Integration, Innovation and Impact. The Panel supported the renewal of IGH’s strategic plan to refresh its ten goals and outline key actions and indicators that build on the work and achievements of the 2013–17 strategic plan. The 2018–23 strategic plan is a relevant and important next step that should be implemented in consultation with the IGH’s incoming IAB.
Recommendation 7: The Panel recommends that IGH’s strategic plan for 2018–23 be launched.
IGH has done an excellent job of drawing researchers involved in more established fields into considering sex and gender in their research but there continues to be a need to attract researchers’ attention to the field of sex and gender science through funding mechanisms. The Panel strongly encouraged the SD to strategically appoint and harness the energy of all IGH Institute Advisory Board (IAB) members to further advance the reach and impact of the institute. Given IGH’s budget, the Panel noted that it will be important for IGH to work with their IAB to identify and develop funding opportunities to attract researchers to the field yet also leverage current IGH investments to continue to build capacity in the field. For example, funding mechanisms could include early career and mid-career investigator awards, research chairs, and team/network grants that target various career stages and also feature awards or stipends for doctoral and postdoctoral trainees. The Panel noted that renewed support to early and mid-career scientists via sex and gender research chairs helps to accelerate research and advance the field of sex and gender science. An integrated approach to attracting researchers and building capacity will increase IGH’s community of researchers and enhance both the application of sex- and gender-based analysis and the success of sex and gender researchers in CIHR’s investigator-initiated funding programs. The Panel supported IGH continuing to provide supplemental grants to integrate sex as a biological variable in biomedical research and to remove barriers to female participation in clinical trials as well as animal research.
The Panel commended IGH for their innovative initiatives to build capacity in and accelerate knowledge translation such as the Hackathon Design Jams, training modules, webinars, and social media training. IGH should continue to invest and take a leadership role in bringing diverse stakeholders together to experiment with innovative knowledge translation initiatives to forge new partnerships with not-for-profit and for-profit organizations. In order to effectively assess the translation and application of sex and gender knowledge into evidence and action, it will be important for IGH, in collaboration with CIHR, to monitor the reach, uptake and impact of activities and investments of the Integration and Innovation strategic directions. For example, in the case of the Integration strategic direction it will important review end-of-grant data to assess the extent to which the plans to integrate sex and/or gender were implemented in the research. On this point, the Panel noted it will be important for CIHR and IGH to monitor and assess the integration of sex and gender considerations across CIHR funding programs as part of CIHR’s SGBA Action Plan.
Recommendation 8: The Panel recommends that IGH be provided the resources necessary to monitor the impacts of their special calls as well as CIHR funded research under the IGH mandate. Specifically, end of grant reports for grants intending to include sex and/or gender considerations should be reviewed to formally assess the investments made toward sex and gender research. In addition, bibliometrics should be collected independently of these report data to provide a baseline from which to measure publication impact and output.
IV. Key Findings
A. Relevance
IGH is the world’s first and only funding institute with a specific focus on sex, gender and health research. The bibliometric analysis confirms that the focus of the institute is relevant; key words associated with this emerging field are increasingly found in publications between 2011 and 2016. Findings demonstrate that Canada is doing well compared to the other top ten countries in the world. The annual number of publication by Canada increased from 51 in 2000 to 201 in 2016. Canada ranked third in the production of publications, and fourth in relation to the quality and impact of journals and relative citations.Footnote 10
IGH’s mandate is to foster research excellence regarding the influence of sex and gender on health and to apply these research findings to identify and address health challenges facing men, women, girls, boys and gender-diverse people. As of 2013, IGH increased its focus on three key priorities with a focus on integrating sex and gender into health research in Canada by consolidating its strategic funding opportunities. They included: 1) Integration; 2) Innovation; and, 3) Impact. In the new strategic plan, the current SD articulates a health ecosystem approach that will move the awareness of sex and gender considerations from its current state to a broader base of government, clinical practice, and the public—into personalized health at the point of care.
IGH’s mandate is directly aligned with and responds to the Government of Canada’s Health Portfolio SGBA Policy, as well as the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans, launched in 2010. Research is aligned with federal partners (e.g., Health Canada, the Social Science and Humanities Research Council of Canada) and provincial partners.
The introduction of the mandatory requirement for all CIHR grant applicants to document sex and/or gender considerations in 2010–11 led to a sharp rise of CIHR investment in IGH mandate because every application that intends to incorporate sex and/or gender is accordingly classified under the IGH mandate. As with all the institutes, the majority of this investment comes from CIHR’s investigator-initiated research program competitions, which are not managed by IGH.
The Government of Canada’s Budget 2018 provided unprecedented support for fundamental research through the three federal granting agencies. For CIHR, this has resulted in an increase to its budget of $354.7 M over 5 years starting in 2018–19. The 2018 Budget responds to Canada's Fundamental Science Review, released in 2017 that stressed the need for significant reinvestment in the federal research ecosystem over a more predictable and better planned multi-year horizon.Footnote 11 Prior to Budget 2018, CIHR’s annual budget had remained relatively stable for approximately the last 10 years, and therefore it was declining substantially in real terms, greatly affecting the ability of researchers to sustain competitive research programs. The majority of CIHR funding under the mandates of the 13 Institutes is investigator-initiated research funding; whereas the Institutes’ strategic research budgetsFootnote 12, which are comparably smaller, are used to catalyze, using strategically placed investments. This newly increased investment in investigator-initiated research could increase CIHR investments that are mapped to IGH’s mandate, and thus may lead to increased demand on IGH to support the Integration of sex and gender by additional investigator-initiated research.Footnote 13
IGH’s mandate and strategic direction continues to build awareness both in why gender and sex should be incorporated into research designs and how to do that in line with CIHR’s Health Research Roadmap II. When investments are broken down by IGH Strategic Priorities, investments in Innovation exceeded those in Integration, suggesting a successful transition from Integration to Innovation. As noted previously, Figure A (in Appendix 3) shows that CIHR investment in Integration rose from $3M to $212M from 2011–12 to 2015–16, decreasing to $193M from 2015–16 to 2016–17. Over this same period, investments classified as Innovation increased from $86M in 2011–12 to $178M in 2015–16, peaking at $288M in 2016–17.
IGH’s contribution to CIHR Initiatives out of its ISI budget increased from 1% in 2011–12 to 24% in 2014–15. Like all other CIHR Institutes, IGH’s contribution to the CIHR Initiatives starting in 2015–16 was mainly via the $4.3M re-allocated to the RAF. However, in 2015–16 and 2016–17, IGH also contributed to CIHR Initiatives from the remaining $4.3M in its ISI budget. This significant increase in investments to CIHR Initiatives in 2015–16 coincides with the beginning of the current SD’s term and the decision to operationalize the Integration priority by making investments in CIHR Initiatives to foster the integration of sex and gender considerations across CIHR themes and priorities.
IGH contributed to eleven cross-cutting multi-institute CIHR initiatives in various capacities. These include: Canadian Consortium on Neurodegeneration in Aging (CCNA), Canadian Longitudinal Study on Aging (CLSA), Dementia Research Strategy (DRS), Canadian Epigenetics, Environment and Health Research Consortium, Global Alliance for Chronic Disease (GACD), Healthy Life Trajectories, Inflammation in Chronic Disease, Pathways to Health Equity for Aboriginal Peoples, Community-Based Primary Health Care (CBPHC), Health and Productive Work (HPW), and Personalized Health.
In addition to reaching out to CIHR at large, IGH successfully reached out to its research, not-for-profit, and industry communities. Stakeholder representatives interviewed commended IGH for consulting them on the Institute’s renewed strategic plan and for the Institute’s extensive community outreach, which helped to build awareness of sex and gender considerations. IGH stakeholders agreed that IGH’s diverse integration initiatives are on point and continue to build capacity in sex and gender integration in health research. An emerging priority as resources permit would be to translate these new methods and methodologies into updated guidelines and manuals for diverse stakeholders (including industry). Key informants to a large extent mentioned the need to deepen conceptualizations of the intersections between sex and gender, noting the value of building incentives for basic scientists and social science researchers to collaborate on this task.
Non-academic research partners interviewed called for increased flexibility for IGH to be able to enter into alternative funding arrangements with diverse partners, referencing the limitation of CIHR processes to forge new partnerships with not-for-profit and for-profit organizations. Further, key informants agreed that there is a need for additional senior level support for the SD to help fulfill CIHR’s SGBA commitments requiring that sex and gender be fully considered and systematically incorporated into policy, programs, and services.
Key informants as well as the Panel agreed that IGH’s mandate continues to be relevant and is sufficiently nimble to lead the development of the emerging field of sex and gender science in Canada and for IGH to lead in this internationally. All lines of evidence align to conclude that there is a continued need to move the field from a current state of awareness of sex and gender considerations towards broader implementation and impact. There continues to be a need to identify and address significant disparities in health-care access and health outcomes for women, men, girls, boys and gender-diverse people. Addressing these disparities requires a better understanding of how gender influences health behavior and health-care utilization, and how sex-based biological factors influence risk factors for disease and response to treatments.
B. Impact
IGH has had strong impact. It has been actively working toward supporting innovative research and advancing knowledge under its mandate and priority research areas. IGH has worked to ensure that research evidence is translated into action that improves health research, services, policies and systems in all IGH strategic initiatives. To achieve this goal, IGH has engaged in advocacy, creating training tools and resources on sex, gender and health research, and citizen engagement.
Knowledge creation and translation highlights in the policy domain include:
- The development of Policy-Research Partnerships (discussed below);
- Setting the standard for caregiver-friendly workplaces that has the potential to enhance work-life balance for carer-employees, improve workforce retention for employers and reduce health-care costs;
- SGBA integration into WHO Zika Virus Guidelines;
- SGBA integration across CIHR and the Government of Canada’s Health Portfolio; and,
- SGBA integration in the Ontario Ministry of Labour granting process.
The Policy-Research Partnerships initiative was developed and launched in partnership with the Health Canada Gender and Health Unit in 2016–17. This initiative is a key activity of Health Canada’s SGBA Action Plan, aimed at funding research-policy partnerships, which will help bridge the gaps between research knowledge and policy development. To date, 5 policy-research partnerships have been funded in the areas of:
- Psychologically healthy workplaces;
- Digital technology to support informal caregivers;
- Cannabis risk perceptions;
- Public education and awareness; and,
- Reorientation of Health Canada Risk Communications for Health Products.
Knowledge creation and translation highlights in the practice domain include:
- The development of Sex and Gender Equity in Reporting (SAGER) Guidelines; and,
- Clinical Practice Guidelines:
- Integration into Canadian Cardiovascular Society Guidelines; and
- Integration into U.S. Preventive Services Task Force recommendations for male infertility, risk assessment, genetic counselling and genetic testing for BRCA-related cancer in women.
Knowledge creation and translation highlights in the public domain include:
- IGH SD featured in CBC’s The Current, Chatelaine, Gazette des Femmes, Wall Street Journal, National Post, Globe and Mail, and Global News;
- The scale up of Men on the Move Model developed by IGH funded research in BC; and
- 3 events that applied design thinking methodology as a novel KT tool:
- Women’s Heart Health Design Jam (2017)
- E-Mental Health Component of Healthy and Productive Work, Work Stress and Wellbeing Hackathon (2017)
- LGBTQI2S Health and Wellness Design Jam (2018).Footnote 14
IGH has led and contributed to several capacity-building initiatives geared to all level of researchers with the purpose of improving awareness, knowledge and self-efficacy of investigators to implement sex- and gender-based analysis in health research. Highlights of IGH capacity building initiatives include:
- Sex and Gender Champions initiative that advocates for mandatory inclusion of individuals with SGBA expertise on research teams for several strategic and priority-driven initiatives;
- Catalyst Grants to integrate sex as a biological variable in biomedical research; and,
- Specialized competency training for researchers and peer reviewers.
From 2010 to 2016, IGH’s investments in capacity building opportunities accounted for an annual average of 24% out of total IGH ISI budget investment ($1.4M per year). The majority of IGH’s investments in capacity building programs was through Training Grants, with an average annual investment of $737K between 2001–02 and 2016–17 (40% of IGH’s capacity building investments annually), followed by Catalyst and Pilot Grant with an annual average investment of $488K (29%), and Training Awards with an annual average of $189K per year (13%). Increased investments in capacity building in 2015–16 and 2016–17 led to improved self-reported awareness, capacity and self-efficacy to implement SGBA.
Another measure of capacity building is to track the number of researchers and trainees funded under IGH’s mandate. The number of researchers funded in IGH’s mandate is directly related to the amount of research investment mapped to IGH’s mandate. As a percentage of total CIHR funded researchers, researchers funded under IGH’s mandate steadily increased from 7% (n=291) in 2000–01 to 70% (n=7,848) in 2015–16, with an average of 55% from 2012–13 to 2015–16. The number of direct trainees funded under IGH’s mandate, as a percentage of the total CIHR-funded direct trainees, ranged from 2% (n=29) in 2000–01 to 42% (n=930) in 2015–16. The maximum (42%) was achieved in 2015–16. Both increases are a result of the CIHR policy requiring applicants to highlight sex and/or gender consideration in their applications; there is a need for monitoring compliance with claimed sex and gender considerations to improve the accuracy of statistics related to the IGH mandate.
All lines of evidence align to conclude that IGH has made progress supporting innovative research and mobilizing knowledge in the policy, clinical practice, and public domains. IGH has developed SGBA expertise on research teams for several strategic and priority-driven initiatives through their Sex and Gender Champion initiative and is currently developing a National Sex and Gender Trainee Network that pairs trainees with mentors at their universities.Footnote 15 One of IGH’s most notable contributions to building capacity of the health research enterprise was achieved through the implementation of their online training modules where researchers and peer reviewers self-report improvements in SGBA awareness, knowledge and self-efficacy. Key informants with extensive knowledge and expertise in SGBA highly recommend their students to take the online trainings, and report learning something new at the various meetings and workshops they attend.
While the proportion of applications with integration of sex and/or gender have increased, there is a continued pressing need to build capacity to integrate and deliver on SGBA considerations in successful CIHR investigator-initiated applications across all pillars (see Figure B in Appendix 3).
The SD was described as a charismatic leader, mentor, and champion for SGBA. Her academic and medical credentials, and her approach has allowed her to influence scientists in the biomedical and clinical fields, demonstrating progress in the uptake of sex differences research in Pillar 1 and 2.
The knowledge translation initiatives such as the Hackathons and Policy-Research Partnerships were described as innovative and promising to advance the emerging field of sex and gender science.
C. Convener and Catalyst
In the last three years, the SD and AD have given over 120 presentations and workshops on the importance of sex and gender to a variety of audiences in Canada and internationally. All lines of evidence demonstrate that IGH has successfully forged collaborations and strengthened networks among the established chairs, centers, and teams supported by IGH initiatives to share information and work together across research areas, disciplines and research pillars. Key informants interviewed for the review commend IGH’s SD and her team for their effective convener and catalyst roles within the scientific community. IGH attended and hosted many investigator meetings of CIHR institutes,Footnote 16 health research forums, and conferences to build awareness of the importance of integrating sex and gender for scientifically excellent and ethical research.
Similarly, IGH has convened one meeting a year with new investigators from CIHR’s Foundation Grant Program to encourage them to consider sex and gender in their research programs. The Institute hosts in-person meetings so that grantees can discuss potential collaborations and engage in discussions about the evaluation of their work. IGH makes a point of highlighting funded work that considers sex and gender on the IGH website and in newsletters. The Institute also worked with its funded researchers to develop fact sheets on important findings in sex and gender science, and has hosted two Best Brains Exchanges during the term of the current SD.
IGH’s convener and catalyst activities successfully leveraged funding to meet the needs of a large and diverse research community. Annual partner contributions to funding opportunities under the IGH mandate steadily increased from $377K to $40.1M from 2001–02 to 2016–17. Partner contributions to funding opportunities funded out of IGH’s budget increased from $37,861 to $3.7M in 2016–17, peaking at $4.1 million in 2015–16 (see Figure D in Appendix 3). When examining partner contributions to opportunities out of IGH’s budget between 2014–15 and 2016–17, the majority of partner contributions to IGH’s initiatives were from not-for-profit organizations and international organizations with an annual average contribution of $1.9M for the former and $727K for the latter.
Contributions from not-for-profit organizations reached its maximum in 2016–17 with $2.2M. International organizations maximum contribution was in 2015–16 ($1.1M). For example, IGH convened with the International Research Community on GENDER-NET, the first European Research Area Network (ERA-NET) and GENDER-NET Plus, an international consortium of sixteen research funders in thirteen countries. From 2001–02 to 2013–14 the majority of partner contributions came from academic partners, with an average contribution of $916K over the 13-year period.
The average annual leverage ratio over IGH’s 16 year period is 0.29. This means for every $100 invested by IGH $29 was leveraged via external partners. After an increase from 0.17 in 2001–02 to 0.28 in 2008–09, the leverage ratio dropped from 2009–10 to 2010–11 followed by a steady increase from 0.27 in 2012–13 to 0.78 in 2016–17 (see Figure E in Appendix 3).Footnote 17
D. Operational Effectiveness
IGH receives $1M annually from CIHR as an Institute Support Grant (ISG) to establish and sustain Institute operating costs and activities. Since 2011–12, IGH spent an annual average of 76% of its ISG budget on Institute Operations and 24% of its ISG budget on Institute Strategic Developments (ISD) (see Figure F in Appendix 3). Further analysis of the ISD reveals that spending on conferences, symposia and workshops accounted for 47% of ISD expenditures, expenditures for professional services averaged 25% and the operation of the Institute-specific IAB, while in operation, accounted for 19% of ISD expenditures. Since 2015–16, IGH has increased its expenditures in the ISD, which is partially attributable to supporting and facilitating Convener and Catalyst activities (e.g., consulting and convening communities, meetings to facilitate collaborations and partnerships) as well as advancing the Institute’s Integration strategy (e.g., SD and AD travel to present at conferences, the development of three interactive online training modules plus their associated annual hosting costs, and scientific meetings and travel costs).
All lines of evidence align to conclude that IGH is using its limited resources well but that IGH has been pushed beyond capacity to fulfill the four components of its mandate. Key informants expressed concern for IGH’s capacity to maintain and build on the momentum generated in the first term of the SD without additional resources. The SD and AD’s consultations, presentations and workshops were described as essential to the support of an emerging field of sex and gender science and ensuring research excellence is being done. IGH has been working with half the funding budget, and half the number of FTEs while leading the design and implementation of CIHR’s SGBA in Health Research Action Plan. The loss of Ottawa-based Institute Staff poses a challenge for IGH considering the number of initiatives under its responsibility and that the current ISG budget is not sufficient to support the required staff.
References
- Government of Canada, Budget 2018 – Equality + Growth: a Strong Middle Class, 2018
- Investing in Canada’s Future: Strengthening the Foundations of Canadian Research. Canada’s Fundamental Science Review (2017)
- Canadian Institutes of Health Research, Shaping Science for a Healthier World: Strategy 2017, [also reffered to as IGH’s 2013–17 strategic plan]
- The Government of Canada invests over $21M in innovative health research
- Overview of the Reforms to CIHR’s Open Suite of Programs: Peer Review Expert Panel
Appendices
Appendix 1: IGH Review Panel Members’ Affiliations and Conflict of Interest Declaration
Chair:
- Gillian Einstein, Wilfred and Joyce Posluns Chair of Women's Brain Health and Aging; Professor, Department of Psychology, University of Toronto; Adjunct Scientist, Women's College Research Institute; Founder, Collaborative Graduate Program in Women's Health, University of Toronto
Panel Members:
- Geert de Vries, Professor, Neuroscience Institute and Associate Vice President for Research & Economic Development, Georgia State University
- Sylvie Mader, Principal Investigator, Molecular Targeting in Breast Cancer Research Unit, IRIC; Professor, Department of Biochemistry, Faculty of Medicine, Université de Montréal
- Cindy Moriarty, Executive Director, Health Programs and Strategic Initiatives, Strategic Policy Branch, Health Canada
- John Oliffe, Professor and Associate Director of Research, School of Nursing, University of British Columbia; Founder and Lead Investigator, University of British Columbia's Men's Health Research program
- Londa Schiebinger, John L. Hinds Professor, History of Science, Stanford University; Director, EU/US Gendered Innovations in Science, Health & Medicine, Engineering and Environment Project
| Panel Member | Conflict of Interest Declaration |
|---|---|
| Gillian Einstein | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Review Panel |
| Geert de Vries | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Sylvie Mader | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Review Panel |
| John Oliffe | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Londa Schiebinger | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Review Panel |
| Cindy Moriarty | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Evaluation Panel |
Appendix 2: Overview of Data Sources and Methods
| Data source | Description |
|---|---|
| Situational Analysis (SA) |
|
| Key informant interviews |
|
| Bibliometric Analysis |
|
Appendix 3: Key Figures
- Figure A: CIHR Investments in IGH’s Mandate by Strategic Priorities
- Figure B: Increase of awareness of sex and gender across CIHR pillars
- Figure C: Investments in Capacity Building out of IGH Budget
- Figure D: Partner Contributions to IGH Funding
- Figure E: Leverage Ratio of Partnerships: Ratio of Partners Investment to IGH Budget Investment
- Figure F: IGH’s Utilization of Institute Support Grant (ISG)
Figure A: CIHR Investments in IGH’s Mandate by Strategic Priorities
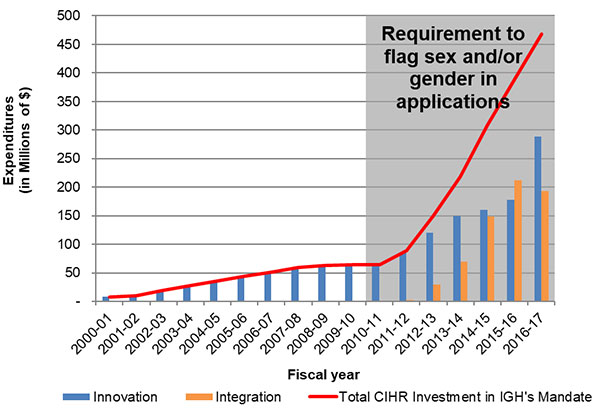
Figure A – Long description
| 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total CIHR Investment in IGH's Mandate | $7,875,115.99 | $10,300,420.60 | $19,280,032.90 | $28,210,403.57 | $36,064,598.18 | $44,187,355.68 | $51,182,999.01 | $59,245,611.10 | $63,573,606.04 | $63,963,814.87 | $63,974,536.72 | $89,281,157.31 | $149,996,334.14 | $218,692,400.33 | $308,465,700.33 | $389,684,077.47 | $467,496,259.62 |
| Innovation | $7,875,115.99 | $10,300,420.60 | $19,280,032.90 | $28,210,403.57 | $36,064,598.18 | $44,187,355.68 | $51,182,999.01 | $59,245,611.10 | $63,573,606.04 | $63,963,814.87 | $63,974,536.72 | $86,341,132.31 | $120,582,394.14 | $149,169,564.33 | $160,409,166.00 | $177,781,178.04 | $288,105,125.64 |
| Integration | $2,940,025.00 | $29,413,940.00 | $69,522,836.00 | $148,056,534.33 | $211,902,899.43 | $193,127,206.98 |
Figure B: Increase of awareness of sex and gender across CIHR pillars Footnote 18
Sex and gender across CIHR pillars
Increase in the proportion of CIHR successful investigator-initiated applications with integration of sex and/or gender (2010 compared to 2016)
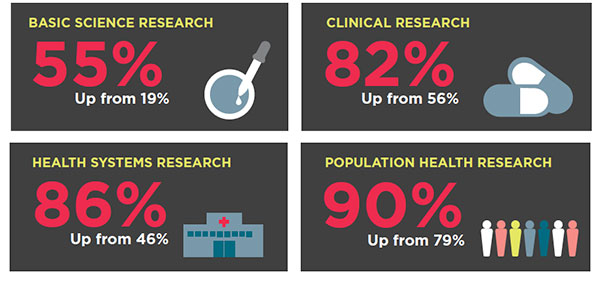
Figure B – Long description
| 2010 | 2016 | |
|---|---|---|
| Basic Science Research | 19% | 55% |
| Clinical Research | 56% | 82% |
| Health Systems Research | 46% | 86% |
| Population Health Research | 79% | 90% |
Figure C: Investments in Capacity Building out of IGH Budget
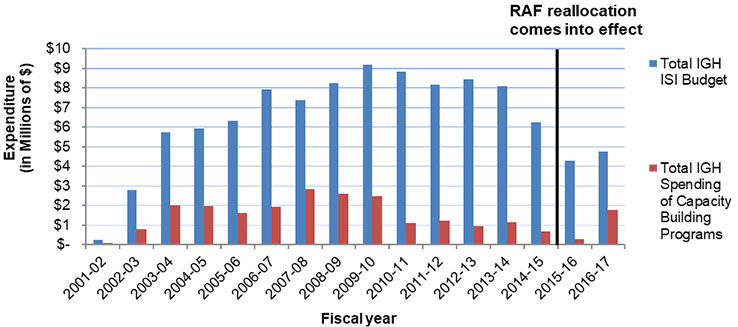
Figure C – Long description
| 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total IGH ISI Budget | $228,830 | $2,779,337 | $5,742,953 | $5,930,412 | $6,306,913 | $7,931,982 | $7,395,054 | $8,238,657 | $9,198,352 | $8,843,295 | $8,172,908 | $8,421,968 | $8,086,360 | $6,247,796 | $4,301,506 | $4,741,615 |
| Total IGH Spending of Capacity Building Programs | $79,557 | $788,772 | $2,020,606 | $1,957,792 | $1,606,275 | $1,921,400 | $2,825,663 | $2,612,735 | $2,470,732 | $1,120,632 | $1,223,327 | $951,191 | $1,147,512 | $670,455 | $295,782 | $1,776,730 |
Figure D: Partner Contributions to IGH Funding
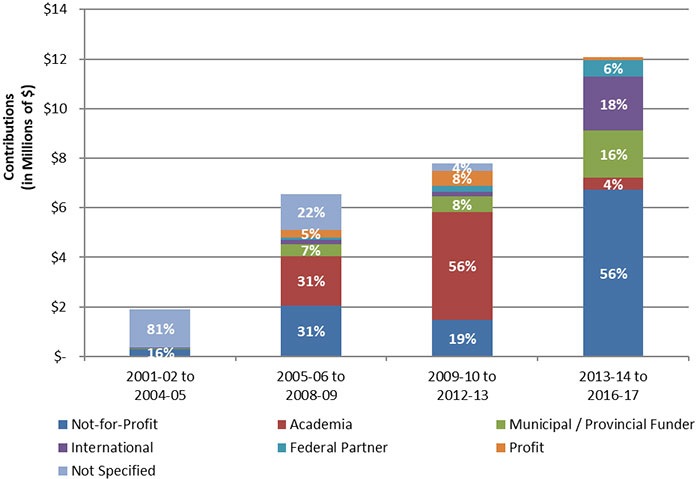
Figure D – Long description
| Partner type | 2001-02 to 2004-05 | 2005-06 to 2008-09 | 2009-10 to 2012-13 | 2013-14 to 2016-17 | ||||
|---|---|---|---|---|---|---|---|---|
| Contributions | Percentage | Contributions | Percentage | Contributions | Percentage | Contributions | Percentage | |
| Not-for-Profit | $304,651.00 | 16% | $2,047,143.00 | 31% | $1,481,437.00 | 19% | $6,729,729.00 | 56% |
| Academia | - | 0% | $2,000,000.00 | 31% | $4,330,000.00 | 56% | $470,000.00 | 4% |
| Municipal / Provincial Funder | $10,000.00 | 1% | $480,054.00 | 7% | $641,950.00 | 8% | $1,903,075.00 | 16% |
| International | $50,000.00 | 3% | $176,660.00 | 3% | $181,313.00 | 2% | $2,180,000.00 | 18% |
| Federal Partner | - | 0% | $85,000.00 | 1% | $258,208.00 | 3% | $682,965.00 | 6% |
| Profit | - | 0% | $307,708.00 | 5% | $587,292.00 | 8% | $100,000.00 | 1% |
| Not Specified | $1,528,260.00 | 81% | $1,442,945.00 | 22% | $300,000.00 | 4% | - | 0% |
Figure E: Leverage Ratio of Partnerships: Ratio of Partners Investment to IGH Budget Investment
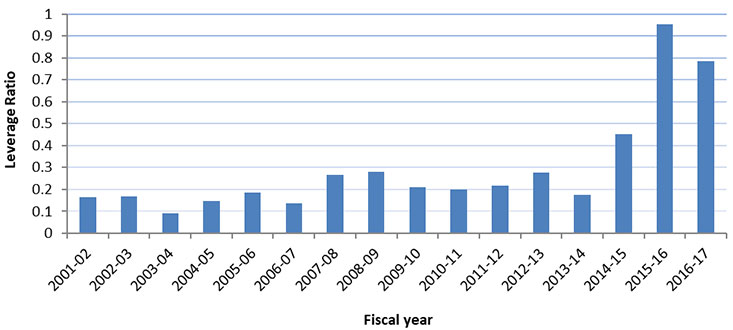
Figure E – Long description
| 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Leverage Ratio | 0.17 | 0.17 | 0.09 | 0.15 | 0.19 | 0.14 | 0.27 | 0.28 | 0.21 | 0.20 | 0.22 | 0.28 | 0.18 | 0.45 | 0.95 | 0.78 |
Figure F: IGH’s Utilization of Institute Support Grant (ISG)
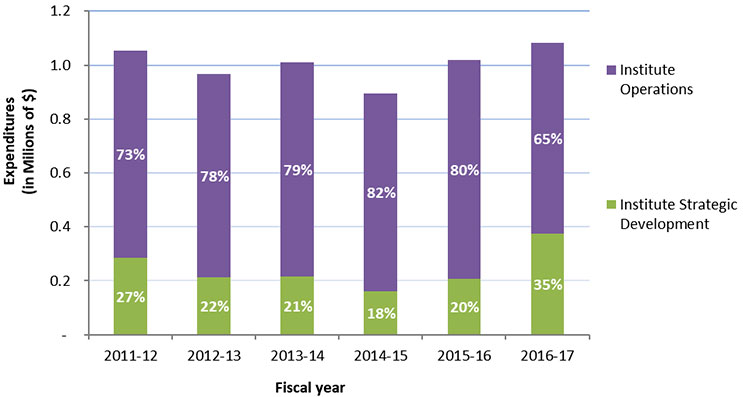
Figure F – Long description
| 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Expenditures | Percentage | Expenditures | Percentage | Expenditures | Percentage | Expenditures | Percentage | Expenditures | Percentage | Expenditures | Percentage | |
| Institute Strategic Development | $284,062 | 27% | $211,675 | 22% | $214,676 | 21% | $160,797 | 18% | $205,804 | 20% | $375,202 | 35% |
| Institute Operations | $769,865 | 73% | $753,752 | 78% | $794,224 | 79% | $733,142 | 82% | $812,745 | 80% | $708,107 | 65% |
Appendix 4: List of IGH Strategic Partners
- Mental Health Commission of Canada
- National Instutes of Health – Office of Research on Women’s Health
- European Association of Science Editors
- Health Canada
- Employment and Social Development Canada
- Social Sciences & Humanities Research Council
- The Netherlands Organization for Health Research and Development (ZonMw)
- National Collaborating Centre for Methods and Tools
- Heart & Stroke Foundation
- Fonds de recherche du Québec - Santé (FRQS)
- Organization for the Study of Sex Differences
- Gender Summit
- Canadian Cardiovascular Society
- Egale Canada
- Canadian Foundation for AIDS Research
- Rainbow Health Ontario
- Brain Canada Foundation
- Ontario HIV Treatment Network
- Memorial University
- Hacking Health
- Institut de recherche Robert-Sauvé en santé et en sécurité du travail
- Cossette Health
- Michael Smith Foundation for Health Research
- Canadian Centre for Occupational Health and Safety
- European Commission – Horizon 2020 European Union funding for Research & Innovation
- Date modified: