Review of the Institute of Aging (IA)
Report of the IA Review Panel
December 2020
At the Canadian Institutes of Health Research (CIHR), we know that research has the power to change lives. As Canada's health research investment agency, we collaborate with partners and researchers to support the discoveries and innovations that improve our health and strengthen our health care system.
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
This publication was produced by the Canadian Institutes of Health Research. The views expressed herein do not necessarily reflect those of the Canadian Institutes of Health Research.
IA Review Panel
Chair: Allison Sekuler, Vice-President, Research, and the Sandra A. Rotman Chair in Cognitive Neurosciece at Baycrest Health Sciences; Professor, Psychology, University of Toronto and Adjunct Professor, Psychology, Neuroscience & Behaviour, McMaster University
Panel Members:
- Edvard Beem, former co-Director of the Netherlands Organisation for Health Research and Development (ZonMw), Chair of the General Assembly of Joint Programming Initiative – More Years, Better Lives
- Verena Menec, Professor, Department of Community Health Sciences, Rady Faculty of Health Sciences, Max Rady College of Medicine, University of Manitoba
- Ben Mortenson, Associate Professor, Department of Occupational Science and Occupational Therapy in the Faculty of Medicine, University of British Columbia
- Nicole Dubuc, Full Professor, School of Nursing in the Faculty of Medicine and Health Sciences at the Université de Sherbrooke and Researcher at the Research Centre on Aging, Université de Sherbrooke
Thanks to all participants in this review and the CIHR IA Review Team: Ian Raskin, Michael Goodyer, Jonathan Gilbert, Sabrina Jassemi, Kim Gaudreau and Emily Guerette.
And special thanks to:
- Dr. Yves Joanette, Scientific Director, IA
- Joanne Goldberg, Assistant Director, IA and
- the IA team
For more information and to obtain copies, please contact: Evaluation@cihr-irsc.gc.ca.
Table of Contents
- Executive Summary
- Overview of the Review
- Observations and Recommendations
- Key Findings
- References
- Appendices
I. Executive Summary
The review of the Institute of Aging (IA) was undertaken by the Canadian Institutes of Health Research (CIHR) as part of the review of the mandate and performance of CIHR Institutes by CIHR’s Governing Council (GC) outlined in the CIHR Act. The review assessed the relevance and performance of IA to inform decisions regarding the role and functioning of the Institute. The review was conducted by the CIHR Evaluation Unit and overseen by a panel of experts in IA’s mandate areas, the IA Review Panel (hereafter referred to as the Panel), who reviewed and interpreted the findings and made the final recommendations. The recommendations and observations of the Panel are summarized below in relation to the two broad issues addressed by the review.
Are changes needed within the current IA mandate in order to address emerging areas of research?
The Panel highlighted the effort of IA during the leadership of the Scientific Director (SD), Dr. Joanette, to accomplish its mandate: “to support research, to promote health aging and to address causes prevention, screening, treatment, support systems and palliation for a wide range of conditions associated with aging”. Given the broad and unique scope of its mandate, IA has worked collaboratively with other Institutes and organizations to address its strategic directions and priorities through initiatives such as the Canadian Longitudinal Study on Aging (CLSA), the Dementia Research Strategy (DRS), Healthy and Productive Work, and eHealth Innovations.
Both Panel discussions and the views of stakeholders emphasized the need for the mandate to incorporate an approach to aging that focuses on wellness and healthspan, as well as on the journey of aging throughout one’s lifetime. The Panel agrees on the importance for IA to build on a holistic approach to aging that includes intersectional, interdisciplinary, and intersectoral considerations at both individual and societal levels for all the roles related to aging in society (e.g., older individuals, caregivers), leveraging interactions to support critical emerging research areas and approaches. The Panel also agrees there is a need for IA to consider the increasing diversity of the aging population and the impact of health equity, health access, social determinants of health, the spectrum of care, and co-morbidities.
Recommendation 1: The Panel recommends framing IA’s mandate with an approach of aging that reflects the potential and opportunity of aging, as well as the unique and positive contributions of older people.
Recommendation 2: The Panel recommends that IA continue developing and implementing an inclusive approach to aging research that incorporates intersectional, interdisciplinary, and intersectorial aspects at both individual and societal levels, recognizing the importance of emerging areas, such as sensory and cognitive issues, big data, and geroscience.
Recommendation 3: The Panel recommends IA continue to consider the impact and highlight the importance of health equity, health access, the social determinants of health, co-morbidities, and the increasing diversity of the aging population in the funding of research in aging to improve the health of aging Canadians (e.g., health promotion/prevention, mobility in aging, social and community engagement, loneliness, active aging, aging in place) and increase the effectiveness of health services and products, and the Canadian health care system.
IA implemented a number of capacity building activities to maintain and strengthen research capacity in its mandate areas including the annual Summer Program on Aging. The Panel sees an opportunity to continue to support capacity building and networking at every career stage, but especially for early and mid-career researchers. There is also a need to build on the previous efforts to continue to build capacity for translating knowledge to clinicians, policy makers, private sector, not-for-profit/charitable sector and the public.
Recommendation 4: The Panel recommends that IA continue to develop innovative initiatives to build capacity at the various career stages with a focus on early and mid-career researchers to support the next generation of aging researchers.
Recommendation 5: The Panel recommends that IA continue to build capacity to translate and mobilize knowledge and technologies to clinicians, policy makers, businesses, and the public to develop more effective products, practices, policies and services, and improve the health care system and health of Canadians.
Given the cross-cutting nature of aging research, the Panel sees it as critical that CIHR’s funding within IA’s mandate should be spread across the four research pillars and include both investigator-initiated research as well as research in priority areas. The Panel is supportive of the current 70/30 split between investigator initiated research and research in priority areas for research in IA’s mandate to support basic research but also enable prioritization to respond to emerging research needs and opportunities. It will be also be important to ensure an appropriate peer review capacity in the field of aging given the need for more research on aging will likely increase based on Canada’s and the world’s demographic.
Recommendation 6: The Panel recommends that CIHR continue to fund aging research across all four CIHR research pillars, ensure there are review panels with a focus and expertise in aging, and maintain the current proportion of funding to approximately 70% investigator-initiated research and 30% research in priority areas to address the crosscutting nature of aging research and to capitalize on emerging research opportunities.
Observations and Recommendations for the Next Scientific Director
The Panel recognizes the current SD’s strong ability to engage, collaborate, and partner with a wide range of stakeholders at the national and international levels has fostered many successful outcomes/partnerships and significantly increased the profile of Canada and Canadian researchers in the aging sector. Coupled with this, IA has organized and participated in numerous workshops, conferences, fora and outreach activities to build awareness, establish connections/relationships and demonstrate leadership. This has allowed for researchers and stakeholders from the public, private, and non-profit sectors to establish the critical partnerships required for IA to achieve its mandate. The Panel notes that the next SD will need to maintain and build on this stakeholder/partnership engagement approach. The Panel considers that the CLSA and the DRS, including the CCNA, are integral to IA’s mandate, and perceives that IA’s leadership of these initiatives remains critical to informing the scientific direction and continued implementation of these flagship initiatives for CIHR. However, the Panel sees a need for IA to ensure that the broader aging research community not directly connected to these initiatives also feel included.
Recommendation 7: The Panel recommends that IA maintain its scientific leadership role for the CLSA and the DRS, while remaining inclusive of and attentive to the broader aging research community not connected to these initiatives.
Recommendation 8: The Panel recommends that the next SD continue to engage with and support the broad aging research community to both maintain and expand partnerships between researchers, funding agencies, knowledge users, the health portfolio organizations, health charities and the private sector at the national and international levels to position Canadian aging researchers as leaders and innovators.
II. Overview of the Review
A. Review Objectives
The review of the Institute of Aging (IA) was conducted by the Canadian Institutes of Health Research (CIHR) as part of a rolling review of the mandate and performance of the 13 CIHR Institutes. The review assessed the relevance and performance of IA to inform future direction and focus of its mandate. The aim of the review is to provide CIHR’s Executive Management and Governing Council (GC) with valid and reliable findings to inform decisions on:
- Whether changes are needed within the current IA mandate to address emerging areas of research; and
- To inform the transition of the Institute to the next Scientific Director (SD).
The review of the IA was overseen by a panel of experts in the IA mandate area who reviewed and interpreted the findings and made the final recommendations. The names and affiliations of the Panel members are listed in Appendix 1. The review was conducted by the CIHR Evaluation Unit to support the work of the Panel.
The review covered the term under the leadership of the current SD, Dr. Yves Joanette, from 2011 and 2018, and includes financial and bibliometric data for the period from 2001 to 2018.Footnote 1 Using a common framework developed for Insitute reviews, the review drew on multiple lines of evidence, including qualitative and quantitative data sources outlined in Appendix 2 with key figures presented in Appendix 3. The review used administrative data on expenditures related to the IA mandate, bibliometric analysis on the ranking of Canada compared to the top countries in the field of aging research, interviews with a number of IA researchers and stakeholder representatives, and the expert opinion and deliberations of the Panel. While each line of evidence has limitations, there is convergence among them to produce key findings. Overall, the results presented provide an accurate account of the Institute’s relevance and performance.
B. CIHR Context and the Canadian Funding Landscape
As outlined in the CIHR Act, the objective of the CIHR is:
“to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system…”
As divisions within CIHR, the institutes are expected to contribute to the achievement of CIHR’s overall objective within their mandate through a number of activities, including: “work in collaboration with the provinces to advance health research and to promote the dissemination and application of new research knowledge to improve health and health services.” As with all of the Institutes, IA supports research across all four of CIHR’s research themes: Biomedical; Clinical; Health Systems and Services; and Social, Cultural, Environmental and Population Health.
The Government of Canada has mandatedFootnote 2 both the Ministers of Health, and Seniors, to make health and aging a priority focus. In the 2017 Mandate Letter to the Minister of Health, “the changing needs of the aging population” was identified as a priority for Ms. Petitpas Taylor. Meanwhile, in the 2018 Minister of Seniors’ Mandate Letter, one of the top priorities identified for Ms. Tassi was to “work with the Minister of Health to engage with stakeholders and parliamentarians on ways to address dementia”. This government focus emphasizes the relevance of supporting research in aging in Canada. The National Strategy for Alzheimer’s Disease and Other Dementias ActFootnote 3 , requires the Minister of Health, in cooperation with representatives of provincial and territorial governments, to develop and implement a comprehensive national dementia strategy. As part of the Government of Canada’s commitment to a National Dementia Strategy, the Minister of Health convened a National Dementia Conference in May 2018 and has established a Ministerial Advisory Board on Dementia.Footnote 4
In terms of funding, the Government of Canada has made significant investments in research and innovation in Budget 2018. For CIHR, this translates to an investment of $354.7M phased in over 5 years and $90.1M ongoing in CIHR’s Investigator-Initiated Research program budgetFootnote 5. The Budget increase follows the final report of the Government of Canada’s Review of Federal Support for Fundamental Science, released on April 10, 2017, which stressed the need for significant reinvestment in the federal research ecosystem over a more predictable and better planned multi-year horizon, as well as improved coordination and collaborations between the three federal granting agencies (CIHR, Natural Sciences and Engineering Research Council of Canada [NSERC], and Social Sciences and Humanities Research Council of Canada [SSHRC]) and the Canada Foundation for Innovation (CFI)Footnote 6. Prior to Budget 2018, CIHR’s budget had been effectively flat for approximately the last 10 years, and therefore it was declining substantially in real terms, greatly affecting the ability of researchers to sustain competitive research programs. CIHR funding of research under the 13 Institute mandates is dominated by CIHR investments in the investigator-initiated operating grant competition compared to the priority-driven grants and awards. The Institute’s budgets are part of the Research in Priority Areas program budget, which enable Institutes to play a catalyst role with strategically placed investments.
C. Institute of Aging Context and Research Landscape
The global population is aging rapidly, and so is Canada’s population. In fact, Canada will join the ranks of super-aged countries (i.e., more than 30% of the population over the age of 60) in 2035Footnote 7. In recent years, the number of Canadians aged 60 and over surpassed the number of those aged 15 and underFootnote 8. This acceleration will continue as baby-boomers, born between 1946 and 1965, reach age 65. Additionally, the number of the “oldest old” (i.e., those aged 85 and over), particularly the centenarians, is growing as never before.
IA’s Mandate, Vision and Mission
Since its inception in 2001, IA has based its mandate on the health and wellness of, as well as the challenges facing, older Canadians. IA’s mandate is “to support research, to promote healthy aging; and to address causes, prevention, screening, diagnosis, treatment, support systems, and palliation for a wide range of conditions associated with aging.” Its goal is to improve the quality of life and health of older Canadians by understanding and addressing or preventing the consequences of a wide range of factors associated with aging.
The current vision of the Institute is to position Canada as a leader in the creation of knowledge through health research that benefits all Canadians and the global community. IA works very closely with all the other 12 CIHR Institutes and is the principal co-leader of a number of key multi-institute initiatives, including the Canadian Longitudinal Study on Aging (CLSA)Footnote 9 and the Dementia Research Strategy (DRS)Footnote 10. IA is a co-lead on the Healthy and Productive Work Initiative and the eHealth Innovations Initiative. IA is also a collaborator in many other inter-institute initiatives, and contributes intensively to the Canadian presence and leadership in a number of international initiatives within its mandate.
IA Strategic Plan (2013-2018)
IA sought to refine its directions and actions even further through its most recent strategic plan for the period from 2013 to 2018. Through a web-based survey and a series of cross-country town hall meetings (the Speaking of Aging Tour), the Institute consulted with over 1,500 researchers, policy makers, industry representatives, representatives from seniors’ organizations, and the public to identify five core strategic priorities. The central goal of IA is to “optimize health and wellness over the entire trajectory of aging for both individuals and society.” As outlined below, the IA’s 2013-2018 Strategic Plan, Living Longer, Living Better, is based on two strategic directions each with two priorities and a fifth enabler priority to guide its activities, funding opportunities, and knowledge translation activities.
1. Strategic Direction 1: Optimizing population health and wellness over the trajectory of aging
1.1. The Life Course Trajectory as a Determinant of Active, and Satisfying Aging: This priority represents a continuation of the emphasis that IA has placed on understanding the determinants of health and wellness in order to identify their impact on active aging and implement programs to prevent illness and promote health.
1.2. Adding Life to the Late Years: IA will support activities aimed at increasing knowledge of the factors and conditions that allow people to not only live longer, but also better while considering the diversity of needs of individuals as well as society.
2. Strategic Direction 2: Addressing the complex health challenges of older adults
2.1. Interventions Appropriate to the Complexity of Older People’s State of Health: A holistic, integrated approach will be taken in developing interventions and pursuing patient-oriented research, particularly to find solutions to neurodegenerative diseases.
2.2. Health Care and Services that Combine and Integrate Continuity, Innovation and Efficiency: The objective of this priority is to develop innovative solutions to make appropriate and efficient health services available, adapt the health care system to older people’s needs, and support various levels with regards to treatment decisions and end-of-life issues (e.g., families, caregivers, professionals, policy makers).
3. Enablers
3.1. Ensuring the Conditions for a Positive Impact on Older People’s Health and Wellness: The final priority differs from the others as it emphasizes the importance of favourable conditions to improve sustainability of research-drive programs, solutions, and models for health and wellness.
III. Observations and Recommendations
A. Are changes needed within the current IA mandate to address emerging areas of research?
1. Panel Observations
The Panel recognizes that the Institute has worked effectively to accomplish its mandate. The IA has co-lead a number of research initiatives such as the CLSA, the DRS (including the CCNA), Healthy and Productive Work, and the eHealth Innovations, all of which directly contribute to its mandate to “support research to promote health aging and to address causes prevention, screening, treatment, support systems and palliation for a wide range of conditions associated with aging.”Footnote 11
IA’s mandate differs from most of CIHR Institutes, by focusing on the aging person in an aging society, and the effects of different diseases and conditions on aging. One of IA’s challenge is to make the broad field of aging researchers and stakeholders feel engaged and supported by the Institute. The stakeholders interviewed confirmed that IA, through initiatives such as CLSA and DRS (including CCNA), has addressed key priorities in the broad field of aging. However, the Panel sees a need for IA to ensure that the broader aging research community not directly connected to these initiatives also feel included.
Throughout the review process, Panel discussions and the views of stakeholders interviewed emphasized that aging is a process and there is need to consider the potential, opportunities, and positive contributions of aging and older people. With this in mind, the Panel sees a need for the mandate to incorporate an approach to aging that focuses on wellness and healthspan, as well as on the journey of aging throughout one’s lifetime.
IA’s current Strategic Plan emphasizes that “the study of aging requires a holistic, interdisciplinary approach and a comprehensive perspective” and that “the entire continuum of services, from prevention to care must be delivered in the context of an integrated, holistic approach”.Footnote 12 The Panel concurs that there is a need to continue to develop and implement a holistic approach to aging that includes intersectional, interdisciplinary, and intersectoral aspects at both individual and societal levels for the persons and organizations working to support aging in society (e.g., older individuals, caregivers). The Panel agrees there is a need to consider the increasing diversity of the aging population. Specifically, IA’s mandate should consider the impact of health equity, health access, social determinants of health, the spectrum of care, co-morbidities as well as the diversity of the aging population. It will be important for IA to build on the leadership role it has played to advance interdisciplinary and intersectional collaborations with the Aging, Seniors and Dementia Division of the Public Health Agency of Canada and with SSHRC in the development of the Healthy and Productive Work initiative.
In support of CIHR’s mandate, IA has the responsibility to build the capacity of the Canadian health research on aging by fostering and supporting the scientific careers of health researchers studying aging. The CIHR 2011 International Review highlighted the necessity for IA to identify the career gaps, and to develop a more long-term plan for supported career tracks of academics working in this area.Footnote 13 The Panel sees an opportunity to continue to support capacity building and networking at every career stage, but especially for early and mid-career researchers, and to build on the previous efforts to continue to build capacity for translating knowledge to clinicians, policy makers, private sector, not-for-profit/charitable sector and the general public.
Just as CIHR broadly funds research across the four research pillars, the Panel agrees that given the cross-cutting nature of aging research, funding within IA’s mandate should be spread across the four research pillars and include both investigator-initiated research as well as research in priority areas. The Panel is supportive of the 70/30 split between investigator initiated research and research in priority areas for research in IA’s mandate, which provides support for important areas of health research and knowledge translation not adequately or optimally addressed by Investigator-Initiated research and maximizes opportunities for collaboration with other Institutes. The Panel also supports IA’s continued use of its Institute-Specific Initiative (ISI) budget to fund the other three research pillars to compensate for the over-representation of biomedical research pillars made through CIHR investments in IA’s mandate. It will be also be important to monitor the implication of the interruption of two IA-specific peer review committees, from 2015-16 to 2017-18, that resulted in a decrease of the annual percentage of CIHR investment in IA’s mandate during this period. This demonstrated the importance of appropriate peer review capacity in the field of aging given the need for more research on aging will likely increase based on Canada’s and the world’s demographic.
The Panel feels that the continued use of multi-Institute and inter-sectoral collaborations by IA will be critical to address emerging areas of research within IA’s mandate. For example, collaborations with other Institutes, government agencies, not-for-profit, charitable and private sector organizations will be a necessary and effective way to leverage resources and expertise to address areas that intersect with critical areas of aging research that should be increasingly supported, such as big data, geroscience, sensory and cognitive issues, policy research, social participation/inclusion, health promotion and prevention, and aging in place. It also will be important for IA to ensure that industry is aware of the research results and works to engage and collaborate with industry to ensure the knowledge translation and mobilizations includes opportunities to move from ideas to innovations to have greatest possible impact on the health of Canadians.
2. Recommendations
Recommendation 1: The Panel recommends framing IA’s mandate with an approach of aging that reflects the potential and opportunity of aging, as well as the unique and positive contributions of older people.
Recommendation 2: The Panel recommends that IA continue developing and implementing an inclusive approach to aging research that incorporates intersectional, interdisciplinary, and intersectoral aspects of aging at both individual and societal levels, recognizing the importance of emerging areas, such as sensory and cognitive issues, big data, and geroscience.
Recommendation 3: The Panel recommends IA continue to consider the impact and highlight the importance of health equity, health access, the social determinants of health, co-morbidities, and the increasing diversity of the aging population in the funding of research in aging to improve the health for aging Canadians (e.g. health promotion/prevention, mobility in aging, social/community engagement, loneliness, active aging, aging in place), and increase the effectiveness of health services and products and the Canadian health care system.
Recommendation 4: The Panel recommends that IA continue to develop innovative initiatives to build capacity at the various career stages, with a focus on early and mid-career researchers to support the next generation of aging researchers.
Recommendation 5: The Panel recommends that IA continue to build capacity to translate and mobilize knowledge and technologies to clinicians, policy makers, businesses, and the public to develop more effective products, practices, policies and services, and improve the health care system and health of Canadians.
Recommendation 6: The Panel recommends that CIHR continue to fund aging research across all four CIHR research pillars, ensure there are review panels with a focus and expertise in aging, and maintain the current proportion of funding to approximately 70% investigator-initiated research and 30% research in priority areas to address the crosscutting nature of aging research and to capitalize on emerging opportunities.
B. Observations for the Next Scientific Director
1. Panel Observations
The Panel recognizes the current SD’s strong ability to engage, collaborate, and partner with a wide range of stakeholders at the national and international levels has fostered many successful outcomes/partnerships and significantly increased the profile of Canada and Canadian researchers in the aging sector. This has allowed for researchers and stakeholders from the public, private, and non-profit sectors to establish the critical partnerships required for IA to achieve its mandate. The Panel notes that the next SD will need to maintain and build on this broad stakeholder/partnership engagement approach, which were widely emphasized and appreciated by partners.
At the international level, the Panel commends Dr. Joanette and IA on the numerous partnerships, including the Alzheimer’s Disease Neuroimaging Initiative, Network of Centres of Excellence on Neurodegeneration, Joint Programme Neurodegenerative Disease Research, Joint Programming Initiative 'More Years, Better Lives', and Global Action Against Dementia. During his tenure, Dr. Joanette has participated in many international partnerships and been a member of numerous international advisory and management boards. For example, he was Chair of the World Dementia Council from February 2016 to March 2018 (and remains a member). He contributed as an international expert to the World Health Organization’s Global Dementia Observatory Reference Guide and maintained a strong connection with the WHO staff in the Department of Aging and in the Department of Mental Health and Dementia. The Panel observes that it will be important for the next SD to possess strong international leadership skills to continue and build on Dr. Joanette’s work to bring Canada, CIHR and IA to the forefront in the fields of aging and dementia research.
At the national level, the SD and Institute have led or supported key initiatives such as the Canadian Longitudinal Study on Aging, the Dementia Research Strategy including the Canadian Consortium Neurodegeneration in Aging, the Canadian Pavilions, the meetings of the Directors of the Canadian Research Centers on Aging, and the Tri-Agency and Health portfolio initiatives such as Healthy and Productive Work and the development of the National Dementia Strategy. The Panel considers that the CLSA and the DRS are integral to IA’s mandate, and perceives that IA’s leadership of these initiatives remains critical to informing the scientific direction and continued implementation of these flagship initiatives for CIHR. In particular, the next SD will need to provide strong leadership to maintain the momentum on these two major initiatives to achieve their objectives and contribute to CIHR’s overall objective. At the same time, it will be important for the next SD to engage, support and include researchers from all areas for aging research across the IA’s mandate.
2. Recommendations
Recommendation 7: The Panel recommends that IA maintain its scientific leadership role for the CLSA and the DRS while remaining inclusive of and attentive to the broader aging research community not connected to these initiatives.
Recommendation 8: The Panel recommends that the next SD continue to engage with and support the broad aging research community to both maintain and expand partnerships between researchers, funding agencies, knowledge users, the health portfolio organizations, health charities and the private sector at the national and international levels to position Canadian aging researchers as leaders and innovators.
IV. Key Findings
A. Relevance
1. Ongoing relevance of the IA mandate
Prior to the creation of CIHR in 2000 and the establishment of IA, there was limited capacity for aging research in Canada. Since its inception, IA has developed and implemented programs designed to build capacity, organize the research community on aging across disciplines and sectors, partner with stakeholders, identify evidence gaps and emerging aging challenges, support innovative research, and work closely with all CIHR Institutes to promote the research on aging within the funding programs and initiatives. As outlined in Section II, the focus of the IA 2013-2018 Strategic Plan is based on two strategic directions composed of two priorities each, with a fifth enabler priority to guide its activities, funding opportunities, and knowledge translation activities.
Investments
CIHR investment in the field of aging research is classified into two categories:
- CIHR investment in IA’s mandate: CIHR’s investment in IA’s mandate refers to all investments, investigator-initiated research and research in priority areas made by CIHR and classified as within IA’s mandate.Footnote 14
- Investment in IA’s Institute-Specific Initiatives: Like each of CIHR’s 13 institutes, IA receives an annual strategic research budget, referred as the Institute-Specific Initiative (ISI). IA’s ISI is under the authority of the institute, and IA can invest it to support a wide array of research activities (e.g., capacity-building initiatives) or to address areas of strategic importance to the Institute that are not be adequately addressed by CIHR’s investments in investigator-initiated research or research in priority areas.
Until 2014-15, the ISI budget per Institute was set at $8.6M. As a result of the Institute Modernization, in 2015-16 and 2016-17 half of each Institutes’ strategic research budgets ($4.3M per year) was reallocated to CIHR’s Roadmap Accelerator Fund (RAF), to support multi-Institute and multidisciplinary initiatives aligned with CIHR’s research priorities patterned along the lines of CIHR’s existing Signature and Strategic Initiatives. The remaining half of the budget remained under the control of Institutes for Institute-Specific Initiatives. As of 2017-18, CIHR ended the RAF, and the Institutes regained control of their full strategic research budgets of $8.6M. However, some of the commitments were for multiple years, so it will take some time for the full budget to be available to IA for Institute-Specific Initiatives. Despite the end of the RAF, it also is expected that the CIHR Institutes will continue to work in collaboration with each other.
Overview of the investments related to IA
Over the past 17 years, the average annual percentage of CIHR investment in IA mandate was 11% of CIHR’s total annual investment. Between the period of 2000-01 and 2009-10, the average annual percentage of CIHR investment in IA increased from 8% to 13% before steadily decreasing to 9% as of 2016-17. The decrease can be partially explained by some methodological changes related to the over-inclusive key words used for the validation exercise, and the redundancy (duplication) in counting projects. The decrease can also be partially explained by the implementation of the new peer review process in 2014-15, which resulted in the abolition of two IA-specific peer review committees—Biological and Clinical Aspects of Aging (BCA), and Social Determinants of Aging (SDA)—both of which were crucial for the support of interdisciplinary projects related to aging research. Similar to CIHR’s core research funding budget, investment in IA’s mandate through investigator-initiated grants/awards averaged 65% over the 16 years period ($59M). In comparison, CIHR’s investment in IA’s mandate through Research in Priority Areas funds averaged 35% over the 18-year period ($31M) (see Appendix 3: Figure 1 ).
Between 2002-03 and 2008-09, IA’s ISI budget had an overall increasing trend ranging between $3.6M and $9.4M Footnote 15.This period was followed by an overall decreasing trend between the years 2009-10 to 2014-15, ranging from $9.4M to $6.6M. Then, starting in 2015-16 and 2016-17, IA’s spending dropped to $3.0M and $4.5M, respectively. This period coincides with the reduction of the ISI budgets from $8.6M to $4.3M. During this period, IA’s ISI spending was less than $4.3M given that IA’s original commitments for these years to CIHR RAF initiatives were greater than $4.3M.Footnote 16 Despite having the full control of their budget, the 2017-18 IA ISI budget available was only $3.9M due to IA’s previous commitments (see Appendix 3: Figure 2).
From 2013-14 to 2017-18, IA’s mandate and ISI investment were made across all five Strategic Priorities. While IA’s ISI investment was mainly in “Health care and services that combine and integrate continuity, innovation and efficiency,” with an annual average of $3M, it ranked 3rd in CIHR investment in IA’s mandate ($31M). CIHR investment in IA’s mandate was mainly in “Interventions appropriate to the complexity of older people’s state of health,” with an annual average of $59M, but it ranked 3rd in IA ISI investment ($2.4M) (see Appendix 3: Figure 3 and Figure 4).
Overall, IA has been engaged in interdisciplinary, integrative health research across all four CIHR themes. Between 2001-02 and 2017-18, investment at both levels related to the field of aging were mainly in Biomedical research. However, during the term of Dr. Yves Joanette, a shift in the distribution of funding per theme of IA’s ISI investment was observed. While maintaining an annual average of 44% at IA’s mandate level, Biomedical investments by IA’s ISI dropped considerably, reaching 4% in 2017-18, and averaging 18% during the term of the current SD. During Dr. Joanette’s tenure, the annual average investment by IA’s ISI increased in the other three themes: Health Systems and Services reached 32% in 2017-18 (13% average); Clinical reached 31% in 2017-18 (9% average); and Social, Cultural, Environmental and Population Health was at 25% in 2017-18, after a high of 31% in 2016-17 (9% average) (see Appendix 3: Figure 5 and Figure 6). Thus, the pattern of IA ISI allocations complemented the investments in IA mandate to ensure some coverage of all themes.
IA also covers the full range of themes in its contributions to several Multi-Institute Collaborations in Signature Initiatives and RAF Initiatives in various capacities (described in more detail in the following section).
IA has a leadership role in the following Initiatives:
- DRS, including the CCNA;
- CLSA;
- Healthy and Productive Work; and
- eHealth Innovations.
IA collaborates with the other Institutes in the following Initiatives:
- Canadian Microbiome 2;
- Personalized Health/Medicine;
- Transitions in Care;
- HIV/AIDS Comorbidities Prevention and Healthy Living;
- Healthy Life Trajectories Initiative (HeLTI); and
- Indigenous Component of HeLTI (I-HeLTI).
IA also financially contributed to the following initiatives from 2011-12 to 2017-18:
- Community-Based Primary Healthcare (CBPHC);
- Canadian Epigenetics, Environment, and Health Research Consortium (CEEHRC);
- Inflammation in Chronic Disease;
- Pathways to Health Equity for Aboriginal Peoples (Pathways); and
- Antimicrobial Resistance (AMR).
The bibliometric analysisFootnote 17 shows considerable growth of Canada’s profile in aging research. Between 2000 and 2017, Canadian researchers published over 31,000 publications within the mandate of IA, with the annual number of publications steadily increasing from 830 in 2000 to 2,772 in 2017. Among the top 10 productive countries, Canada is ranked 7thFootnote 18 in all five aging priority areas (see Appendix 3: Figure 7).Footnote 19 When considering the population of the top 10 most productive countries, Canada is ranked 1st among countries with a population of less than 50 M. During the same period, the Specialization Index (SI)Footnote 20 shows that Canada is more specialized across the five priority areas as whole, compared to the world average. In fact, Canada ranks 5th amongst the top 10 countries for the SI of publications (see Appendix 3: Figure 10). Additionally, when measuring whether Canadian researchers publish in journals with a high Impact Factor, Canada ranked 4th for the Average Relative Impact FactorFootnote 21 (ARIF) (see Appendix 3: Figure 8). The number of citations received by a published paper also is well above the world average: Canada ranked 2nd for the Average Relative CitationsFootnote 22 (ARC) (see Appendix 3: Figure 9). Regarding collaboration, Canada is ranked 3rd in inter-institutional collaboration, and 2nd in international collaboration for the five priority areas (see Appendix 3: Figure 11 and Figure 12).
Findings across all lines of evidence indicate that IA has met its overarching mandate. In particular, Interviewees emphasized the key role that IA played in leading and supporting key initiatives (e.g., the DRS, CCNA, and CLSA) and advised continuing the momentum fostered through these initiatives. Furthermore, IA has been successful creating and fostering partnerships, both within Canada and internationally. Interviewees also mentioned the SD has been a strong advocate of aging by increasing its impact within CIHR as well as with other Institutes. Suggestions from interviewees include further consideration of advancing and translating knowledge, as well as supporting research and capacity that consider the broader physical, mental, and social factors of the aging process (e.g. social determinants of health, sensory processes).
B. Impact
1. Knowledge Advancement and Translation Activities
Under the tenure of the current SD, IA has supported and led a number of major research initiatives and projects advancing and translating knowledge in the field of aging research. The CLSA and DRS are associated with the Institute as the major initiatives in addressing IA’s strategic directions.
Strategic Direction 1: Optimizing population health and wellness over the trajectory of aging
Major Initiative: the Canadian Longitudinal Study on Aging
The CLSA is a national, longitudinal research platform that has recruited participants from all ten Canadian provinces, and is collecting data on wide-ranging areas, such as the medical, social, psychological, lifestyle, and economic aspects of people’s lives, along with biological samples that will support numerous aging-related research questions. As of 2015, the recruitment and data collection were completed for the 51,338 participants, aged 45-85 at enrolment. To date, CLSA has retained most of its participants with a retention rate of 94.5%. The participants are separated in two complementary cohorts that may be studied separately or together:
- The Tracking cohort of 21,241 participants randomly selected from within all ten provinces who are interviewed by telephone; and
- The Comprehensive cohort of 30,097 participants randomly selected from within 25-50 km of 11 data collection sites (in seven provinces) who are interviewed in-person, take part in in-depth physical assessments at data collection sites, and provide blood and urine samples.
The CLSA platform is designed to support the collection, preparation, and release of data and biospecimens to build capacity for high-quality research on aging in Canada and internationally. CLSA also has prioritized the availability of data for trainees specifically by implementing a policy to provide raw data free of charge for those completing graduate theses or postdoctoral research. Over 160 co-investigators, including theme leads and site leads, contributed to the initial design and content of the CLSA and continue to provide ongoing support.
Since 2016, more than 124 research teams have accessed the data, an additional 60 research teams have been engaged in conducting methodological projects using the CLSA platform, and more than 15 research papers have been published using CLSA data. The topics of CLSA projects range from those that are focused on a specific aspect of aging (e.g. lung function) to those that are more comprehensive in scope (e.g. health and social inequity).
Additional Initiatives
Also under the strategic direction: “Optimizing population health and wellness over the trajectory of aging,” IA has led Canada’s participation in the European Joint Programming Initiative “More Years, Better Lives” since 2015 in partnership with the Institute of Health Service and Policy Research, as well as the Social Sciences and Humanities Research Council. The Institute also co-led the Healthy and Productive Work initiative, and participated in the Canadian Microbiome Initiative 2.
Strategic Direction 2: Addressing the complex health challenges of older adults
Major Initiative: CIHR Dementia Research Strategy
The DRS aims to support research on the latest preventive, diagnostic, and treatment approaches to Alzheimer's disease and other neurodegenerative diseases causing dementia. Featuring international and national components, the DRS allows the Government of Canada to support world-class research on dementia that will contribute to the global pursuit of finding a cure or disease-modifying treatment for dementia by 2025. The objectives of the DRS are to:
- Create new scientific knowledge and enable its translation into improved health and wellness of people living with dementia, their families and their caregivers; and
- Ensure collaborative Canadian participation and leadership towards world-class research that is aligned with a coordinated and global agenda in order to address the complex challenges of dementia.
To date, this component has enabled Canada and Canadian researchers to participate in the following key international research initiatives:
- Alzheimer’s Disease Neuroimaging Initiative (ADNI) (United States): ADNI unites researchers with study data as they work to define the progression of Alzheimer’s disease. Through the DRS, CIHR supports four ADNI Canadian Centres.
- Network of Centres of Excellence on Neurodegeneration (CoEN) (Canada and 8 European countries): This initiative aims to encourage collaborative research between recognized national centres of excellence in neurodegeneration in order to accelerate progress in understanding the mechanisms of disease, as well as the identification of new therapeutic approaches. Since 2011, 11 projects involving Canadian researchers were funded.
- Joint Programme Neurodegenerative Disease Research (JPND) (European Union Initiative with 27 partner countries, including Canada): JPND is the largest global research initiative aimed at tackling the challenge of neurodegenerative diseases. JPND aims to increase coordinated investments between participating countries in research aimed at finding causes, developing cures, and identifying appropriate ways to care for those with neurodegenerative diseases. Since 2012, 13 projects have involved Canadian researchers.
The national component of DRS includes:
- Canadian Consortium Neurodegeneration in Aging (CCNA): Launched in 2014-15, the CCNA benefit from a permanent, ongoing $5M/year budget commitment from the Government of Canada. The goal of the CCNA is to support a collaborative, integrated, strategically oriented, bold, transformative, and highly impactful research and knowledge translation on Alzheimer's disease and other neurodegenerative diseases in aging having an impact on cognition. CCNA brings together more than 350 clinicians and researchers who work among 20 pan-provincial teams throughout Canada to accelerate progress in age-related neurodegenerative diseases, including Alzheimer’s disease, Vascular dementia, Frontotemporal dementia, and Lewy body dementia (among others). The CCNA teams draw on the data and support eight national platforms. They are also supported by four cross-cutting programs that are integrated throughout the activities of the teams: Women, Gender, Sex and Dementia (WGSD), Knowledge Translation and Exchange (KTE), Training and Capacity Building (TCB), and, Ethical, Legal, and Social Issues (ELSI). In terms of other impacts to date, review of the CCNA Progress Reports submitted to CIHR indicate that the CCNA has:
- Published approximately 110 publications between 2014 and 2017;
- Produced 387 scientific presentations and 114 knowledge translation activities directed at the general public;
- Considered sex and/or gender in research, with 18 of 20 teams indicating that issues of sex/gender are being factored into their experiments/analysis;
- Included indigenous considerations in four of seven teams;
- Established and strengthened partnerships with international collaborators: 14 of 20 teams report the formation of new partnerships, with a total of 42 international researchers/entities; and
- Transformed the collaborative way research on dementia is done in Canada.
- New Directions in Dementia
- Team Grant: Big Data on Dementia (2016): In partnership with the Institute of Neurosciences, Mental Health and Addiction (INMHA), the objectives of this funding opportunity were to: support the generation and enrichment of Canadian big datasets on neurodegenerative diseases and support the access, linkage, analysis, and dissemination of Big Data on dementia in Canada and internationally. One project was funded with $4.75M over 5 years.
- Operating Grant: Social Inclusion of Individuals with Dementia and Carers (2016): In partnership with INMHA and the Alzheimer Society of Canada, the objectives of this funding opportunity were to support research projects focused on: improving the social inclusion of those living with dementia and/or their carers – “living better with dementia”; and, identifying and evaluating scalable relevant interventions having an impact on social inclusion at the individual or population levels. Four grants with total of $1.2M over 4 years were funded.
- Operating Grant: Challenge of Dementia in Indigenous Populations (2016): In partnership with INMHA and the Institute of Indigenous Peoples’ Health, the aim of this funding opportunity was to build capacity among Indigenous and non-Indigenous scholars or students in the area of dementia research. Two grants received a total of $1M over 5 years in funding.
- The Wilfred and Joyce Posluns Chair in Women’s Brain Health and Aging: In partnership with INMHA, the Institute of Gender and Health, the Ontario Brain Institute, the Posluns Family, and the Alzheimer Society of Canada, the objective of this funding opportunity was to support a leading researcher based at an Ontario institution to develop and implement a Chair with the goal of impacting and enhancing research on sex and gender differences in brain health and aging. The Chair was awarded to Dr. Gillian Einstein one of Canada’s leading experts in the field of neuroscience, sex, and gender. As Chair, Dr. Einstein has:
- Leveraged funding over $1.3M for her research;
- Engaged with 8 health system/care practitioners/professionals, 3 community advisory members, 145 patients enrolled, 17 researchers/academics and 12 trainees;
- Published 3 peer-reviewed journal articles and 3 book chapters;
- Participated in 26 presentations; and
- Been involved in 6 national articles in mass media or interviews and 10 international articles in mass media or interviews.
Additional Initiatives
Under the strategic direction “Addressing the complex health challenges of older adults”, IA has also co-led the eHealth Innovation initiative, which funded 13 aging-related teams out of the 19 funded teams. The Institute has also been active in the following: Late-Life Issues initiative, which supported two teams since April 2016; the Geroscience initiative, which was launched in August 2018; the Personalized Health initiative; and the Transitions in Care, in which IA leads the Understanding the Health Impact of Inactivity for the Benefit of Older Adults and Astronauts component in partnership with the Canadian Space Agency.
2. Contributions to Building Capacity
With regards to the enabling Strategic Priority, “Ensuring the Conditions for a Positive Impact on Older People’s Health and Wellness”, IA delivers the well-received annual Summer Program in Aging (SPA), an advanced research training program that crosses disciplines, sectors, institutions, and geographical boundaries and addresses one or more of the IA’s priority research themes. SPA is open to graduate students and post-doctoral fellows involved in research on aging, as well as those doing post-graduate clinical training with a research component in aging. The program is composed of plenary lectures and interactive workshops on topics such as peer review, grant proposal writing, interdisciplinarity, research communication, and knowledge translation. Since 2006, IA has co-hosted twelve SPAs, in partnership with research centers on aging across Canada, and has engaged more than 540 masters, doctoral, and postdoctoral trainees. Overall findings from the recent SPA assessment indicate that SPA is:
- Strategically built around a focused topic area each year, allowing for capacity-building in research that aligns with one of IA's strategic priorities and initiatives;
- A training platform for CIHR best practices (e.g., grant writing, peer review, sex- and gender-based analysis (SGBA));
- Increasingly known as Canada's elite training program in aging research;
- Resulting in alumni who are now in positions where they can mentor their own trainees and send them to a SPA;
- A valuable networking tool for collaborations with international agencies, researchers, and trainees;
- Increasingly known internationally, which allows for possibilities for collaboration on an international level for trainees who have participated in a SPA; and
- IA’s flagship training program.
From 2001 to 2018, IA’s ISI annual investments in capacity building accounted on average for 34% of its budget. These include investments in catalyst/pilot programs, training grants and awards, and development grants (see Appendix 3: Figure 13). During the same period, 9% of total CIHR funded direct traineesFootnote 23 and 14% of indirect traineesFootnote 24 were funded under IA’s mandate (see Appendix 3: Figure 14 and Figure 15). However, the reporting of CLSA and CCNA trainees (direct and indirect) is reported on separately and therefore not included in the percentage above. As per the 5th Progress Report of CCNA (December 2017), there were 214 documented CCNA-affiliated trainees reported by researchers. This includes trainees not directly funded by the CCNA but engaged in a CCNA research project. With respect to CLSA, 47 trainees accessed CLSA data between 2014 and 2018. Regarding the researchers funded under IA’s mandate, they represent 19% of total CIHR funded researchers between 2001 and 2018 (see Appendix 3: Figure 16). Of which, on an annual average, 70% were mid-career and senior researchers at the IA’s mandate and ISI investment. Meanwhile, the early career researchers were funded in a proportion of 12% (see Appendix 3: Figure 17).
With regards to knowledge translation and engagement with the public, it is worth noting that CIHR’s very first Café Scientifique was focused on aging, and IA has since organized numerous Café Scientifiques. In addition, IA partnered with Dementia Care Alliance of the University of Waterloo and the Alzheimer Society to present Cracked: an innovative research-based play that follows persons with dementia and their families on their unique journeys with dementia, from diagnosis to their new lives in long-term care.
Findings from stakeholder interviews suggest three overarching themes. The first is that IA has successfully supported capacity building amongst senior researchers. Examples include supporting the funding of research Chairs. The second theme is that, although SPA supports trainees, there is a gap in the support of early and mid-career researchers. Here, CIHR’s Project Grant program was cited as excellent example of supporting capacity building in this area, but it was suggested additional capacity building opportunities for researchers in early stages of their career (e.g., mentorship, networking, grants) should be created, along with additional, broader, training opportunities for trainees beyond specialized topics in the SPA. The third theme is that IA should build on its successes to date to further advance knowledge translation to professionals, decision makers, and the public to improve visibility of Canada’s aging research beyond academia.
C. Convener and Catalyst
1. Contribution of Scientific Leadership to the Convener-Catalyst Role
IA has used a variety of networking and stakeholder engagement approaches to help bring together various aging stakeholders, ranging from creating stakeholder alliances and international partnership opportunities, to hosting meetings and symposia as part of IA-led strategic initiatives. All lines of evidence indicate that Dr. Joanette has been a true leader in the convener and catalyst role.
Beginning in 2014, IA has developed a unique collaboration with Canadian partner organizations and other CIHR Institutes by coordinating a Canadian-branded common exhibit space at international conferences known as the “Canadian Pavilion.” In addition to the Canadian Pavilion, IA also established a tradition of hosting Networking Events for Canadian participants and international partners, in collaboration with its partners at international conferences since 2014. Stakeholder interviewees suggested that both approaches have significantly increased the visibility of Canadian aging research around the world.
Beginning under the leadership of the previous SD, and continuing today, IA convened the meeting of the Directors of the Canadian Research Centers on Aging on a semi-annual basis to have an opportunity to exchange best practices and encourage collaboration.
In the context of CCNA, IA initiated a novel approach with the CCNA’s First Partners’ Forum. The purpose of this forum was to provide a platform for researchers, partners, and other stakeholders to exchange information and to allow those stakeholders to provide feedback that ultimately will contribute to shaping the full application for the CCNA.
Complementary to the international initiatives mentioned in previous sections, the Institute has sought to engage with international partners and stakeholders to provide researchers on aging and dementia the opportunity to establish international collaborations for joint learning opportunities and establish a critical mass to advance the knowledge base in aging.
Canada and France cohosted the second Global Action Against Dementia legacy event in 2014 through CIHR, led by IA and the French National Alliance for Life and Health Sciences (Aviesan). Nearly 200 industry leaders, academia, and policy makers from across Canada and around the world met in Ottawa. The ultimate goal was to propose practical solutions for the development and support of joint public-private, international approaches to dementia research.
Under the leadership of IA and the Institute of Health Services and Policy Research, and in partnership with two Networks of Centres of Excellence (NCE) – AGE-WELL and the Canadian Frailty Network – CIHR became the official Canadian representatives in the European Union’s (EU) Active and Assisted Living Program. AGE-WELL aims to help older Canadians maintain their independence, health and quality of life through technologies and services that increase their safety and security, support their independent living, and enhance their social participation. The Panel believes it will be important for IA to support and encourage technology related research and knowledge mobilization when AGE-WELL completes its NCE funding in February 2020, should it not be renewed through 2023.Footnote 25
IA has hosted various public events that facilitate informal public discussions and exchanges on topics related to aging. IA has also fostered dissemination on emerging research and topics related to aging through media interviews, newsletters, bulletins, and journal articles. Since 2011, IA’s Scientific Director, Dr. Joanette has completed over 31 interviewsFootnote 26 for radio, print newspapers, and television in English and French. From 2016 to 2018, IA has circulated 21 newsletters as well as 35 funding opportunities. Furthermore, IA has authored nine articles in the Canadian Journal on Aging in addition to various other publications in international journals. During the current SD’s tenure, the Institute organized or attended more than 450 meetings. Between 2011 and 2018, the Institute held 15 Institute Advisory Board meetings; organized or attended 129 Conferences, Seminars, and Workshops; and convened close to 20 meetings with stakeholders to discuss and exchange upon the 2013-2018 Strategic Plan. IA has also conducted and prepared numerous meetings regarding CIHR initiatives. In fact, IA was involved in over 165 events related to DRS; 13 for CLSA; 9 for eHealth Innovations; 5 for Healthy and Productive Work; and 41 regarding other CIHR initiatives. IA also hosted the first “outside of Europe” Management Board meetings for the EU Joint Programme on Neurodegenerative Disease Research (JPND) and the Joint Programming Initiative on More Years, Better Lives (JPI-MYBL). On average, IA was engaged in 65 meetings per year between 2012 and 2018.
2. Involvement of the Scientific Director
Dr. Joanette has maximized opportunities to further advance the cause of aging and dementia. Dr. Joanette was a key witness for the Canadian Senate Standing Committee on Social Affairs, Science and Technology (SOCI) Committee, which focused on the challenges of dementia in Canada. Dr. Joanette actively participated in the planning of the “National Dementia Forum,” and is currently actively involved in the development of the National Dementia Strategy. From February 2016 to March 2018, Dr. Joanette chaired the World Dementia Council, and he currently remains a member of the Council. Additionally, IA is a member of many international advisory and management boards, including several European initiatives in which Canada participates, including the EU Joint Programme on Neurodegenerative Disease Research. He is a member of the following: Steering Committee of the Joint Programming Initiative: More Years, Better Lives; Advisory Board of the Milken Institute’s Centre for the Future of Ageing; and Global Council on Brain Health. He contributed as an international expert for the development of the Global Dementia Observatory Reference Guide from the World Health Organization. He participated in shaping Canada’s contribution to the Global Action Plan on Dementia (adopted by the World Health Assembly). In addition, he maintained a strong international presence with the staff of the World Health Organization in the Department of Aging and in the Department of Mental Health and Dementia.
3. Partnering to Achieve CIHR and Institute Objectives
IA partnerships and collaborations with other entities took several forms, such as collaborating and convening to enable knowledge exchange and networks of researchers and practitioners, raising more research funding, as well as increasing the capacity within specific areas. Partner organizations include all of the other CIHR Institutes, along with government agencies and departments, international partners, and not-for-profit organizations, such as health charities (see Appendix 4).
IA has been very successful at leveraging partner contributions to funding opportunities funded from their ISI budget. The leverage ratio between 2001-02 and 2017-18 was 0.44, which means for every $100 invested out of IA’s budget there is $44 leveraged from external partners. During the current SD’s tenure, the average ratio was 0.88, and there was a steep increase in 2015-16 to 2.05. The leverage ratio decreased in 2016-17 and 2017-18, yet remained above 1.0 (See Appendix 3: Figure 18 and Figure 19 ).
D. Operational Effectiveness
The Institution within which IA operates receives $1M annually from CIHR as an Institute Support Grant (ISG). Over the period ranging from 2011-12 to 2017-18, IA has spent an average of 97% of its annual ISG allotment. The remaining 3% of the ISG allotment for each year, plus the funds received from partners to reimburse the costs of strategic and collaborative activities throughout each fiscal year, has resulted in an accumulated surplus of approximately $446K as of the end of the 2017-18 fiscal year (see Appendix 3: Figure 20). IA has allowed the accumulation of the surplus over the years in order to ensure sufficient funding for the final four months of its mandate, a period for which the estimated expenditures will exceed the annual ISG allotment. Between 2011-12 and 2016-17, IA spent an annual average of 71% on Institute Operations (which include staff salary) and the remainder was used for Institute Strategic Development (ISD) (see Appendix 3: Figure 21). Further analysis of the Institute Strategic Development expenditures reveals that 78% was used for conferences, symposia, and workshops led by IA (see Appendix 3: Figure 22).
During the term of Dr. Joanette, CIHR changed the nature and the extent of the support it provides to the Institutes. Prior to July 2015, the Institutes were supported by full-time Ottawa-based Institute Staff (OBIS). This support was composed of individuals who worked for Institutes but were situated at CIHR’s headquarters in Ottawa. In the case of IA, this represented two full-time employees. As part of the Institute Modernization introduced in 2014 by CIHR’s Governing Council, it was decided that the Ottawa-based Institute Staff would be replaced with the Integrated Institute Teams (IIT). This matrix management model of integrated teams comprised of staff from various Branches across CIHR Portfolios that provide functional support to each Institute as a part of the integrated team. Each IIT team member works with multiple Institutes. The workload of the Institute increased significantly with the implementation of these changes with an unchanged ISG budget. In order to partially mitigate this additional workload, IA hired an additional employee (0.8 FTE) in 2015.
IA is composed of an SD, four employees and a consultant. Since Dr. Yves Joanette started as the SD of IA, the Institute has retained talent within its staff and has successfully minimized turnover.
E. Summary
In summary, the Panel commends the IA for its exceptional support and growth of the aging research community in Canada. Over the last review period, Canada’s profile and reputation in aging and health research has been strong and continues to increase globally. Significant new ventures have been developed to maintain the postitive trajectory in the years to come, and the IA is known for its strong support of trainees through programs like the SPA. The SD should be commended for his role in overseeing IA’s success. He is recognized as highly collaborative and has been a leader both nationally and internationally, which has helped bring Canada to the forefront in aging and health research, particularly in the area of dementia.
V. References
- Government of Canada, Budget 2018
- Investing in Canada’s Future: Strengthening the Foundations of Canadian Research. Canada’s Fundamental Science Review (2017) [ PDF (8.25 MB) - external link ]
- CIHR, Health Research Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians, Strategic Plan 2014-15 – 2018-18
- CIHR 2011 International Review – Expert Review Team Report for Institute of Aging
- CIHR, IA, Strategic Plan 2013-2018: Living Longer, Living Better
- CIHR, IA, Mandate
- AGE-WELL
VI. Appendices
Appendix 1: IA Review Panel Members’ Affiliations and Conflict of Interest Declaration
Chair:
- Allison Sekuler, Vice-President, Research, and the Sandra A. Rotman Chair in Cognitive Neurosciece at Baycrest Health Sciences; Professor, Psychology, University of Toronto and Adjunct Professor, Psychology, Neuroscience & Behaviour, McMaster University
Panel Members:
- Edvard Beem, former co-Director of the Netherlands Organisation for Health Research and Development (ZonMw), Chair of the, General Assembly of Joint Programming Initiative – More Years, Better Lives
- Verena Menec, Professor, Department of Community Health Sciences, Rady Faculty of Health Sciences, Max Rady College of Medicine, University of Manitoba
- Ben Mortenson, Associate Professor, Department of Occupational Science and Occupational Therapy in the Faculty of Medicine, University of British Columbia
- Nicole Dubuc, Full Professor, School of Nursing in the Faculty of Medicine and Health Sciences at the Université de Sherbrooke and Researcher at the Research Centre on Aging, Université de Sherbrooke
| Panel Member | Conflict of Interest Declaration |
|---|---|
| Allison Sekuler | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Edvard Beem | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Verena Menec | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Ben Mortenson | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
| Nicole Dubuc | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Review Panel |
Appendix 2: Overview of Data Sources and Methods
| Data source | Description |
|---|---|
| Situational Analysis (SA) |
|
| Key informant interviews |
|
| Bibliometric Analysis |
|
Appendix 3: Key Figures and Tables
- Figure 1: Annual Percentage of CIHR investment in IA’s mandate
- Figure 2: IA Institute-Specific Initiative (ISI) Budget Spending
- Figure 3: CIHR Investment in IA’s mandate Strategic Priorities
- Figure 6: IA ISI Investment in IA Strategic Priorities
- Figure 5: CIHR Investment in IA Mandate: Percentage of Theme
- Figure 6 : Investissements du budget de recherche stratégique de l’IV, par thème (en pourcentage)
- Figure 7: Number of Publications
- Figure 8: Average Relative Impact Factor
- Figure 9: Average of Relative Citations
- Figure 10: Specialization Index
- Figure 11: Inter-Institutional Collaboration
- Figure 12: International Collaboration
- Figure 13: Investment in Capacity Building out of IA’s ISI Budget
- Figure 14: Percentage of Direct Trainees Funded under IA’s Mandate
- Figure 15: Percentage of Indirect Trainees Supported under IA’s Mandate
- Figure 16: Percentage of Funded Researchers under IA’s mandate
- Figure 17: Percentage of Funded Researchers under IA’s mandate by career stage
- Figure 18: Leverage Ratio of Partnerships: Partners to Investments out of IA’s ISI Budget
- Figure 19: Leverage Ratio of Partnerships: Partnership Contributions and IA’s ISI Budget
- Figure 20: ISG Funding
- Figure 21: Percentage of the Utilization of ISG Funds
- Figure 22: Institute Strategic Development Expenditures 2011-12 to 2017-18
Figure 1: Annual Percentage of CIHR investment in IA’s mandate
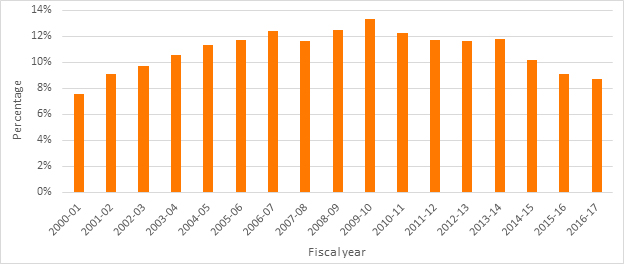
Figure 1 – Long Description
| 2000-2001 | 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Percentage | 8% | 9% | 10% | 11% | 11% | 12% | 12% | 12% | 12% | 13% | 12% | 12% | 12% | 12% | 10% | 9% | 9% |
Figure 2: IA Institute-Specific Initiative (ISI) Budget Spending
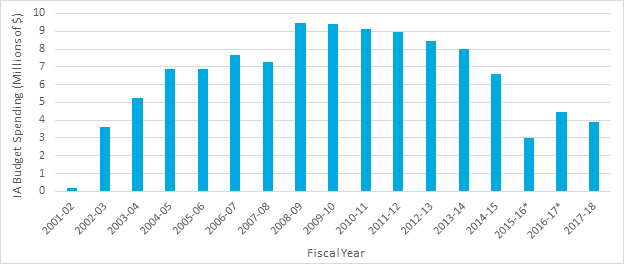
Figure 2 – Long Description
| 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016* | 2016-2017* | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Budget Spending | $ 179,920.00 | $ 3,594,950.84 | $ 5,251,047.62 | $ 6,862,980.76 | $ 6,854,087.82 | $ 7,669,434.45 | $ 7,274,972.80 | $ 9,445,238.60 | $ 9,378,935.71 | $ 9,144,510.00 | $ 8,944,293.11 | $ 8,432,944.00 | $ 7,997,049.00 | $ 6,605,118.62 | $ 3,021,131.00 | $ 4,466,653.00 | $ 3,877,566.52 |
Figure 3: CIHR Investment in IA’s mandate Strategic Priorities
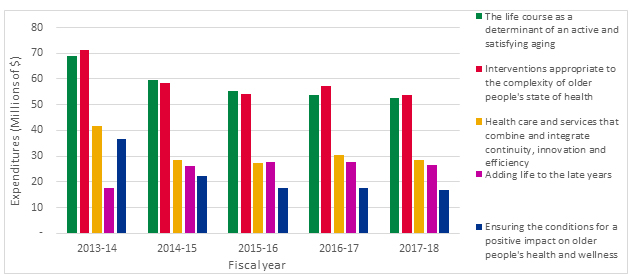
Figure 3 – Long Description
| Strategic Priorities | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 |
|---|---|---|---|---|---|
| The life course as a determinant of an active and satisfying aging | $ 54,266,535.00 | $ 68,956,317.80 | $ 59,401,457.65 | $ 55,231,516.00 | $ 53,864,779.00 |
| Interventions appropriate to the complexity of older people's state of health | $ 48,483,705.00 | $ 71,077,117.80 | $ 58,579,902.00 | $ 54,102,315.00 | $ 57,318,832.00 |
| Health care and services that combine and integrate continuity, innovation and efficiency | $ 26,432,610.00 | $ 41,739,039.00 | $ 28,481,586.62 | $ 27,385,935.00 | $ 30,231,049.00 |
| Adding life to the late years | $ 14,263,766.00 | $ 17,518,668.00 | $ 25,978,792.65 | $ 27,731,670.00 | $ 27,504,244.00 |
| Ensuring the conditions for a positive impact on older people's health and wellness | $ 22,157,271.00 | $ 36,771,769.80 | $ 22,219,908.27 | $ 17,710,258.00 | $ 17,682,968.00 |
Figure 4: IA ISI Investment in IA Strategic Priorities
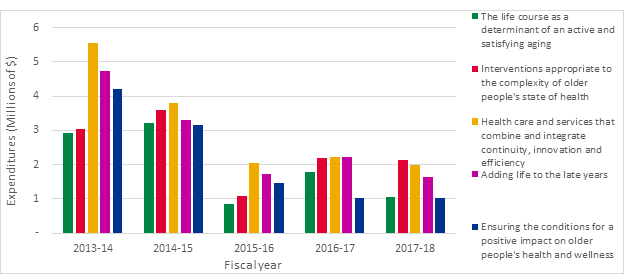
Figure 4 – Long Description
| Strategic Priorities | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 |
|---|---|---|---|---|---|
| The life course as a determinant of an active and satisfying aging | $ 68,956,317.80 | $ 59,401,457.65 | $ 55,231,516.00 | $ 53,864,779.00 | $ 52,481,603.00 |
| Interventions appropriate to the complexity of older people's state of health | $ 71,077,117.80 | $ 58,579,902.00 | $ 54,102,315.00 | $ 57,318,832.00 | $ 53,628,101.00 |
| Health care and services that combine and integrate continuity, innovation and efficiency | $ 41,739,039.00 | $ 28,481,586.62 | $ 27,385,935.00 | $ 30,231,049.00 | $ 28,381,528.00 |
| Adding life to the late years | $ 17,518,668.00 | $ 25,978,792.65 | $ 27,731,670.00 | $ 27,504,244.00 | $ 26,416,130.52 |
| Ensuring the conditions for a positive impact on older people's health and wellness | $ 36,771,769.80 | $ 22,219,908.27 | $ 17,710,258.00 | $ 17,682,968.00 | $ 16,914,476.52 |
Figure 5: CIHR Investment in IA Mandate: Percentage of Theme
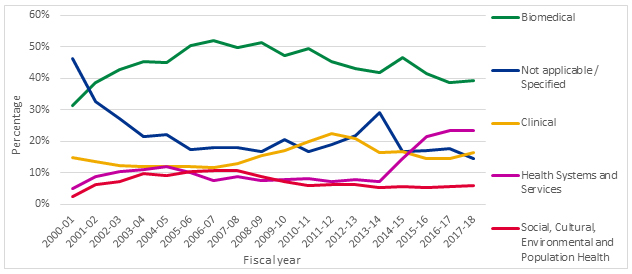
Figure 5 – Long Description
| Themes | 2000-2001 | 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biomedical | 31% | 39% | 43% | 45% | 45% | 50% | 52% | 50% | 51% | 47% | 49% | 45% | 43% | 42% | 47% | 41% | 39% | 39% |
| Not applicable / Specified | 46% | 32% | 27% | 22% | 22% | 17% | 18% | 18% | 17% | 21% | 17% | 19% | 22% | 29% | 17% | 17% | 18% | 15% |
| Clinical | 15% | 14% | 12% | 12% | 12% | 12% | 12% | 13% | 15% | 17% | 20% | 23% | 21% | 16% | 17% | 15% | 14% | 17% |
| Health Systems and Services | 5% | 9% | 10% | 11% | 12% | 10% | 8% | 9% | 8% | 8% | 8% | 7% | 8% | 7% | 14% | 22% | 23% | 23% |
| Social, Cultural, Environmental and Population Health | 3% | 6% | 7% | 10% | 9% | 10% | 11% | 11% | 9% | 7% | 6% | 6% | 6% | 5% | 6% | 5% | 6% | 6% |
Figure 6: IA ISI Investment: Percentage of Theme
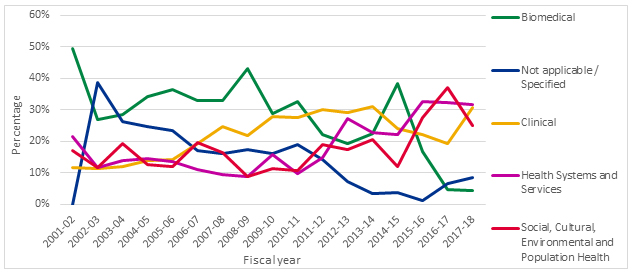
Figure 6 – Long Description
| Themes | 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biomedical | 50% | 27% | 28% | 34% | 36% | 33% | 33% | 43% | 29% | 33% | 22% | 19% | 22% | 38% | 17% | 5% | 4% |
| Not applicable / Specified | 0% | 39% | 26% | 25% | 23% | 17% | 16% | 17% | 16% | 19% | 14% | 7% | 3% | 4% | 1% | 7% | 9% |
| Clinical | 12% | 11% | 12% | 14% | 14% | 19% | 25% | 22% | 28% | 28% | 30% | 29% | 31% | 24% | 22% | 19% | 31% |
| Health Systems and Services | 22% | 12% | 14% | 14% | 14% | 11% | 10% | 9% | 16% | 10% | 15% | 27% | 23% | 22% | 33% | 32% | 32% |
| Social, Cultural, Environmental and Population Health | 17% | 12% | 19% | 13% | 12% | 20% | 17% | 9% | 11% | 11% | 19% | 17% | 21% | 12% | 28% | 37% | 25% |
Figure 7: Number of Publications
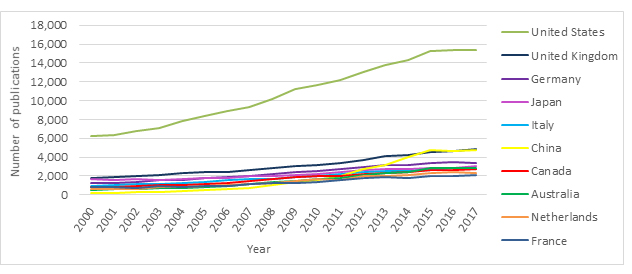
Figure 7 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| United States | 6,278 | 6,327 | 6,802 | 7,109 | 7,821 | 8,410 | 8,941 | 9,317 | 10,198 | 11,182 | 11,634 | 12,225 | 12,985 | 13,813 | 14,332 | 15,269 | 15,323 | 15,325 | 193,291 |
| United Kingdom | 1,825 | 1,929 | 1,981 | 2,143 | 2,285 | 2,395 | 2,372 | 2,664 | 2,823 | 3,076 | 3,138 | 3,408 | 3,705 | 4,124 | 4,215 | 4,567 | 4,671 | 4,825 | 56,146 |
| Germany | 1,209 | 1,291 | 1,403 | 1,589 | 1,571 | 1,782 | 1,832 | 2,030 | 2,151 | 2,402 | 2,543 | 2,723 | 2,963 | 3,117 | 3,123 | 3,378 | 3,426 | 3,406 | 41,939 |
| Japan | 1,690 | 1,575 | 1,641 | 1,610 | 1,654 | 1,798 | 1,767 | 1,987 | 1,987 | 2,130 | 2,214 | 2,426 | 2,660 | 2,777 | 2,768 | 2,845 | 2,838 | 3,036 | 39,403 |
| Italy | 936 | 1,012 | 1,112 | 1,176 | 1,266 | 1,348 | 1,533 | 1,626 | 1,707 | 1,832 | 2,010 | 2,148 | 2,379 | 2,543 | 2,556 | 2,642 | 2,787 | 2,706 | 33,319 |
| China | 157 | 224 | 274 | 323 | 431 | 526 | 577 | 758 | 985 | 1,310 | 1,543 | 1,952 | 2,711 | 3,206 | 4,026 | 4,714 | 4,652 | 4,798 | 33,167 |
| Canada | 830 | 865 | 909 | 991 | 1,064 | 1,135 | 1,288 | 1,506 | 1,631 | 1,831 | 1,977 | 2,036 | 2,213 | 2,347 | 2,376 | 2,591 | 2,643 | 2,772 | 31,005 |
| Australia | 507 | 579 | 599 | 696 | 729 | 821 | 914 | 1,095 | 1,330 | 1,409 | 1,648 | 1,783 | 2,056 | 2,303 | 2,453 | 2,788 | 2,832 | 2,833 | 27,375 |
| Netherlands | 643 | 636 | 615 | 797 | 851 | 970 | 1,061 | 1,188 | 1,286 | 1,485 | 1,634 | 1,609 | 1,979 | 2,040 | 2,140 | 2,358 | 2,381 | 2,271 | 25,944 |
| France | 770 | 785 | 755 | 891 | 853 | 924 | 925 | 1,102 | 1,270 | 1,291 | 1,363 | 1,565 | 1,744 | 1,854 | 1,795 | 2,010 | 1,988 | 2,100 | 23,985 |
Figure 8: Average Relative Impact Factor
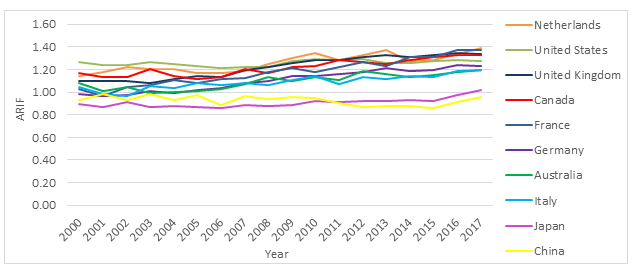
Figure 8 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 1.15 | 1.18 | 1.22 | 1.20 | 1.20 | 1.17 | 1.16 | 1.19 | 1.25 | 1.30 | 1.35 | 1.28 | 1.32 | 1.37 | 1.27 | 1.28 | 1.33 | 1.39 | 1.28 |
| United States | 1.26 | 1.24 | 1.24 | 1.26 | 1.25 | 1.23 | 1.22 | 1.22 | 1.22 | 1.28 | 1.29 | 1.28 | 1.29 | 1.26 | 1.26 | 1.28 | 1.28 | 1.28 | 1.26 |
| United Kingdom | 1.10 | 1.10 | 1.10 | 1.08 | 1.12 | 1.14 | 1.13 | 1.19 | 1.22 | 1.26 | 1.28 | 1.28 | 1.31 | 1.33 | 1.31 | 1.33 | 1.34 | 1.33 | 1.25 |
| Canada | 1.17 | 1.13 | 1.13 | 1.21 | 1.14 | 1.11 | 1.14 | 1.21 | 1.17 | 1.22 | 1.23 | 1.28 | 1.27 | 1.24 | 1.28 | 1.31 | 1.33 | 1.33 | 1.24 |
| France | 1.03 | 0.96 | 1.04 | 1.06 | 1.11 | 1.08 | 1.11 | 1.12 | 1.17 | 1.22 | 1.18 | 1.22 | 1.27 | 1.23 | 1.31 | 1.31 | 1.37 | 1.37 | 1.22 |
| Germany | 0.98 | 0.97 | 0.97 | 1.01 | 0.99 | 1.01 | 1.04 | 1.08 | 1.10 | 1.14 | 1.14 | 1.16 | 1.18 | 1.21 | 1.18 | 1.19 | 1.24 | 1.23 | 1.13 |
| Australia | 1.08 | 1.01 | 1.05 | 0.99 | 1.00 | 1.01 | 1.03 | 1.07 | 1.14 | 1.10 | 1.13 | 1.11 | 1.18 | 1.16 | 1.13 | 1.15 | 1.18 | 1.20 | 1.13 |
| Italy | 1.04 | 0.99 | 0.97 | 1.06 | 1.03 | 1.08 | 1.06 | 1.08 | 1.07 | 1.10 | 1.14 | 1.07 | 1.13 | 1.11 | 1.14 | 1.13 | 1.19 | 1.20 | 1.11 |
| Japan | 0.89 | 0.87 | 0.91 | 0.87 | 0.88 | 0.87 | 0.86 | 0.88 | 0.88 | 0.89 | 0.92 | 0.92 | 0.92 | 0.92 | 0.93 | 0.92 | 0.97 | 1.02 | 0.92 |
| China | 0.93 | 0.99 | 0.93 | 0.99 | 0.93 | 0.97 | 0.89 | 0.97 | 0.94 | 0.96 | 0.94 | 0.90 | 0.87 | 0.88 | 0.88 | 0.86 | 0.91 | 0.96 | 0.91 |
Figure 9: Average of Relative Citations
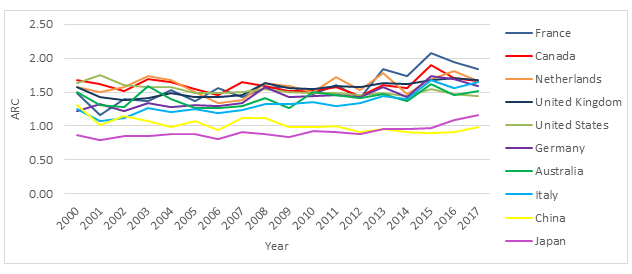
Figure 9 – Long Description
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| France | 1.48 | 1.16 | 1.40 | 1.37 | 1.52 | 1.36 | 1.56 | 1.43 | 1.56 | 1.59 | 1.47 | 1.60 | 1.42 | 1.84 | 1.73 | 2.08 | 1.94 | 1.84 | 1.64 |
| Canada | 1.67 | 1.62 | 1.51 | 1.69 | 1.65 | 1.55 | 1.45 | 1.64 | 1.58 | 1.52 | 1.52 | 1.57 | 1.44 | 1.61 | 1.56 | 1.90 | 1.70 | 1.66 | 1.61 |
| Netherlands | 1.57 | 1.50 | 1.58 | 1.74 | 1.67 | 1.49 | 1.34 | 1.38 | 1.64 | 1.59 | 1.50 | 1.72 | 1.52 | 1.77 | 1.47 | 1.70 | 1.81 | 1.66 | 1.61 |
| Royaume-Uni | 1.58 | 1.42 | 1.38 | 1.40 | 1.49 | 1.43 | 1.43 | 1.46 | 1.63 | 1.56 | 1.55 | 1.59 | 1.57 | 1.64 | 1.61 | 1.67 | 1.71 | 1.68 | 1.57 |
| United States | 1.63 | 1.75 | 1.61 | 1.58 | 1.57 | 1.49 | 1.49 | 1.50 | 1.54 | 1.50 | 1.49 | 1.49 | 1.46 | 1.48 | 1.44 | 1.54 | 1.47 | 1.44 | 1.51 |
| Germany | 1.21 | 1.32 | 1.22 | 1.34 | 1.28 | 1.31 | 1.29 | 1.34 | 1.58 | 1.42 | 1.44 | 1.46 | 1.42 | 1.57 | 1.43 | 1.73 | 1.69 | 1.58 | 1.47 |
| Australia | 1.49 | 1.31 | 1.28 | 1.59 | 1.39 | 1.27 | 1.27 | 1.29 | 1.42 | 1.26 | 1.50 | 1.45 | 1.42 | 1.47 | 1.36 | 1.62 | 1.45 | 1.51 | 1.43 |
| Italy | 1.25 | 1.07 | 1.11 | 1.26 | 1.21 | 1.24 | 1.19 | 1.24 | 1.33 | 1.33 | 1.35 | 1.29 | 1.33 | 1.45 | 1.39 | 1.67 | 1.56 | 1.65 | 1.38 |
| China | 1.30 | 1.02 | 1.15 | 1.08 | 0.98 | 1.08 | 0.94 | 1.11 | 1.12 | 0.98 | 0.99 | 1.00 | 0.92 | 0.95 | 0.91 | 0.90 | 0.91 | 0.99 | 0.96 |
| Japan | 0.86 | 0.79 | 0.86 | 0.85 | 0.87 | 0.88 | 0.81 | 0.91 | 0.88 | 0.84 | 0.93 | 0.92 | 0.88 | 0.96 | 0.95 | 0.98 | 1.08 | 1.15 | 0.93 |
Figure 10: Specialization Index
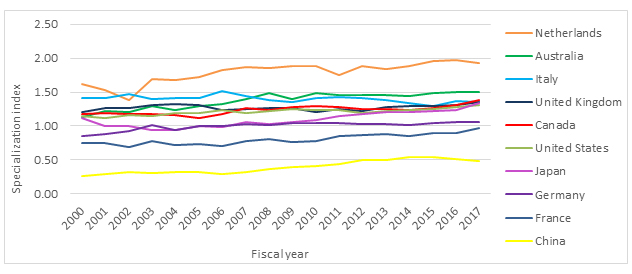
Figure 10 – Long Description
| Country | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 1.61 | 1.53 | 1.39 | 1.68 | 1.68 | 1.73 | 1.82 | 1.87 | 1.85 | 1.89 | 1.89 | 1.75 | 1.89 | 1.84 | 1.88 | 1.96 | 1.98 | 1.92 | 1.84 |
| Australia | 1.13 | 1.22 | 1.20 | 1.29 | 1.24 | 1.30 | 1.32 | 1.39 | 1.49 | 1.40 | 1.49 | 1.45 | 1.45 | 1.46 | 1.44 | 1.48 | 1.50 | 1.50 | 1.44 |
| Italy | 1.42 | 1.42 | 1.47 | 1.40 | 1.41 | 1.41 | 1.52 | 1.44 | 1.39 | 1.36 | 1.41 | 1.43 | 1.40 | 1.38 | 1.34 | 1.30 | 1.37 | 1.35 | 1.39 |
| United Kingdom | 1.20 | 1.27 | 1.27 | 1.30 | 1.32 | 1.30 | 1.23 | 1.25 | 1.26 | 1.27 | 1.21 | 1.25 | 1.22 | 1.28 | 1.29 | 1.29 | 1.30 | 1.35 | 1.27 |
| Canada | 1.17 | 1.19 | 1.18 | 1.17 | 1.17 | 1.11 | 1.18 | 1.26 | 1.24 | 1.27 | 1.30 | 1.27 | 1.25 | 1.26 | 1.23 | 1.27 | 1.31 | 1.38 | 1.25 |
| United States | 1.14 | 1.12 | 1.16 | 1.14 | 1.19 | 1.19 | 1.23 | 1.19 | 1.22 | 1.25 | 1.23 | 1.23 | 1.19 | 1.22 | 1.23 | 1.25 | 1.28 | 1.30 | 1.21 |
| Japan | 1.11 | 1.01 | 1.01 | 0.94 | 0.94 | 0.99 | 0.98 | 1.06 | 1.03 | 1.06 | 1.09 | 1.15 | 1.18 | 1.20 | 1.21 | 1.22 | 1.24 | 1.33 | 1.08 |
| Germany | 0.86 | 0.88 | 0.92 | 1.01 | 0.95 | 1.00 | 1.00 | 1.03 | 1.02 | 1.05 | 1.04 | 1.05 | 1.03 | 1.03 | 1.02 | 1.04 | 1.06 | 1.06 | 1.01 |
| France | 0.75 | 0.74 | 0.69 | 0.78 | 0.72 | 0.73 | 0.70 | 0.78 | 0.81 | 0.77 | 0.78 | 0.85 | 0.87 | 0.88 | 0.85 | 0.89 | 0.89 | 0.96 | 0.81 |
| China | 0.26 | 0.30 | 0.32 | 0.30 | 0.32 | 0.31 | 0.29 | 0.32 | 0.36 | 0.40 | 0.41 | 0.44 | 0.50 | 0.50 | 0.54 | 0.55 | 0.51 | 0.49 | 0.48 |
Figure 11: Inter-Institutional Collaboration
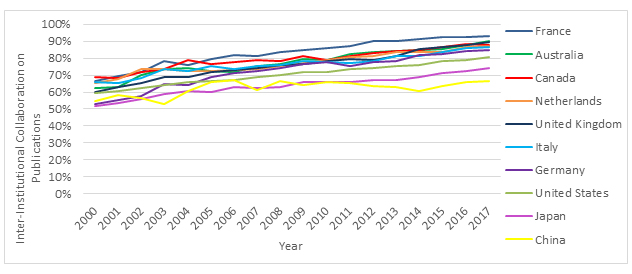
Figure 11 – Long Description
| Country | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| France | 67% | 70% | 72% | 78% | 76% | 80% | 82% | 81% | 83% | 85% | 86% | 87% | 90% | 90% | 91% | 93% | 93% | 93% | 86% |
| Australia | 63% | 63% | 70% | 74% | 74% | 72% | 72% | 75% | 76% | 79% | 79% | 82% | 84% | 84% | 85% | 85% | 88% | 90% | 81% |
| Canada | 69% | 68% | 72% | 73% | 79% | 77% | 78% | 79% | 78% | 81% | 79% | 81% | 83% | 84% | 85% | 86% | 88% | 88% | 81% |
| Netherlands | 65% | 68% | 74% | 74% | 73% | 73% | 73% | 74% | 75% | 77% | 79% | 81% | 81% | 84% | 84% | 83% | 87% | 87% | 80% |
| United Kingdom | 60% | 63% | 65% | 69% | 69% | 72% | 73% | 74% | 76% | 76% | 78% | 79% | 79% | 81% | 85% | 87% | 88% | 89% | 78% |
| Italy | 66% | 65% | 68% | 73% | 73% | 75% | 73% | 75% | 76% | 78% | 78% | 77% | 78% | 81% | 81% | 84% | 86% | 87% | 78% |
| Germany | 53% | 55% | 58% | 65% | 64% | 69% | 71% | 73% | 74% | 77% | 78% | 76% | 78% | 78% | 82% | 83% | 84% | 84% | 75% |
| United States | 59% | 61% | 63% | 64% | 66% | 67% | 67% | 69% | 70% | 72% | 72% | 74% | 74% | 75% | 76% | 78% | 79% | 80% | 72% |
| Japan | 52% | 53% | 56% | 59% | 61% | 60% | 63% | 62% | 63% | 66% | 66% | 66% | 67% | 67% | 69% | 71% | 73% | 74% | 65% |
| China | 55% | 58% | 57% | 53% | 61% | 66% | 67% | 61% | 66% | 64% | 66% | 65% | 63% | 63% | 61% | 63% | 66% | 66% | 64% |
Figure 12: International Collaboration
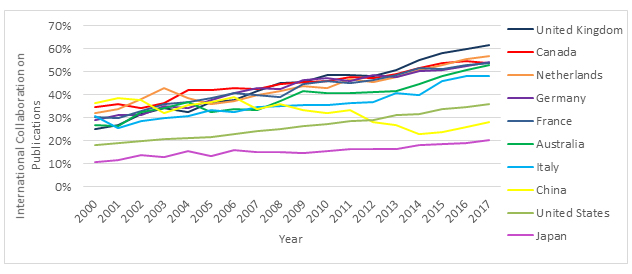
Figure 12 – Long Description
| Country | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011-2017 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| United Kingdom | 25% | 27% | 32% | 34% | 32% | 37% | 38% | 41% | 45% | 45% | 48% | 49% | 48% | 51% | 55% | 58% | 60% | 62% | 47% |
| Canada | 34% | 36% | 34% | 36% | 42% | 42% | 43% | 42% | 45% | 46% | 46% | 48% | 47% | 49% | 52% | 54% | 55% | 54% | 47% |
| Netherlands | 32% | 34% | 38% | 43% | 38% | 36% | 37% | 40% | 42% | 44% | 43% | 47% | 45% | 48% | 51% | 53% | 55% | 57% | 46% |
| Germany | 29% | 31% | 31% | 35% | 34% | 38% | 41% | 43% | 43% | 46% | 47% | 46% | 48% | 48% | 50% | 51% | 53% | 54% | 45% |
| France | 30% | 30% | 33% | 36% | 37% | 38% | 41% | 40% | 39% | 44% | 46% | 45% | 46% | 49% | 52% | 51% | 53% | 54% | 45% |
| Australia | 27% | 26% | 32% | 34% | 37% | 32% | 34% | 33% | 37% | 41% | 41% | 41% | 41% | 42% | 45% | 48% | 51% | 53% | 42% |
| Italy | 31% | 25% | 29% | 30% | 31% | 33% | 32% | 35% | 35% | 36% | 35% | 36% | 37% | 41% | 40% | 46% | 48% | 48% | 38% |
| China | 36% | 38% | 38% | 32% | 35% | 37% | 39% | 34% | 36% | 34% | 32% | 33% | 28% | 27% | 23% | 24% | 26% | 28% | 28% |
| United States | 18% | 19% | 20% | 21% | 21% | 22% | 23% | 24% | 25% | 26% | 27% | 29% | 29% | 31% | 32% | 34% | 35% | 36% | 28% |
| Japan | 11% | 12% | 14% | 13% | 15% | 13% | 16% | 15% | 15% | 15% | 16% | 17% | 16% | 17% | 18% | 18% | 19% | 20% | 16% |
Figure 13: Investment in Capacity Building out of IA’s ISI Budget
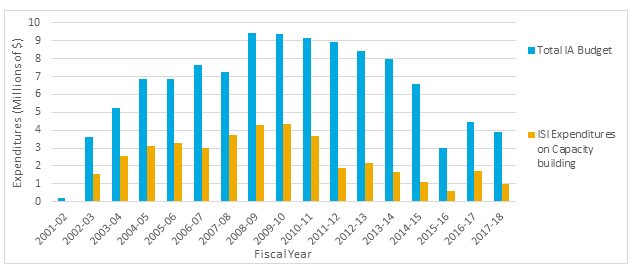
Figure 13 – Long Description
| 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total IA Budget | $ 179,920.00 | $ 3,594,950.84 | $ 5,251,047.62 | $ 6,862,980.76 | $ 6,854,087.82 | $ 7,669,434.45 | $ 7,274,972.80 | $ 9,445,238.60 | $ 9,378,935.71 | $ 9,144,510.00 | $ 8,944,293.11 | $ 8,432,944.00 | $ 7,997,049.00 | $ 6,605,118.62 | $ 3,021,131.00 | $ 4,466,653.00 | $ 3,877,566.52 |
| ISI Expenditures on Capacity building | $ 15,334.00 | $ 1,568,251.84 | $ 2,547,086.62 | $ 3,131,636.76 | $ 3,289,604.82 | $ 3,011,743.45 | $ 3,732,580.80 | $ 4,267,521.60 | $ 4,335,581.71 | $ 3,682,280.00 | $ 1,910,218.11 | $ 2,146,282.00 | $ 1,682,156.00 | $ 1,110,932.62 | $ 576,695.00 | $ 1,702,054.00 | $ 1,004,498.52 |
Figure 14: Percentage of Direct Trainees Funded under IA’s Mandate
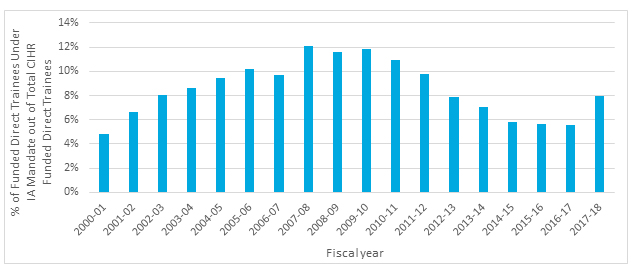
Figure 14 – Long Description
| 2000-2001 | 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % of Funded Direct Trainees Under IA Mandate out of Total CIHR Funded Direct Trainees | 5% | 7% | 8% | 9% | 9% | 10% | 10% | 12% | 12% | 12% | 11% | 10% | 8% | 7% | 6% | 6% | 6% | 8% |
Figure 15: Percentage of Indirect Trainees Supported under IA’s Mandate
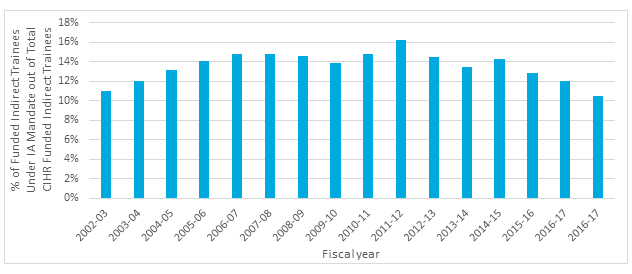
Figure 15 – Long Description
| 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % of Funded Indirect Trainees Under IA Mandate out of Total CIHR Funded Indirect Trainees | 11% | 12% | 13% | 14% | 15% | 15% | 15% | 14% | 15% | 16% | 14% | 13% | 14% | 13% | 12% | 11% |
Figure 16: Percentage of Funded Researchers under IA’s mandate
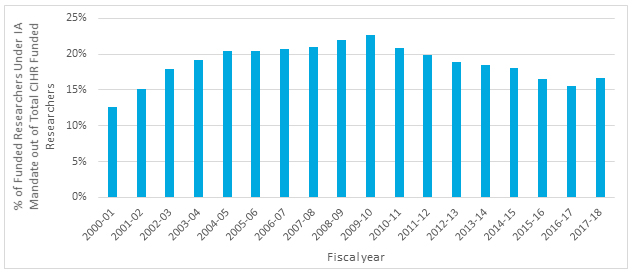
Figure 16 – Long Description
| 2000-2001 | 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % of Funded Researchers Under IA Mandate out of Total CIHR Funded Researchers | 13% | 15% | 18% | 19% | 20% | 20% | 21% | 21% | 22% | 23% | 21% | 20% | 19% | 18% | 18% | 17% | 16% | 17% |
Figure 17: Percentage of Funded Researchers under IA’s mandate by career stage
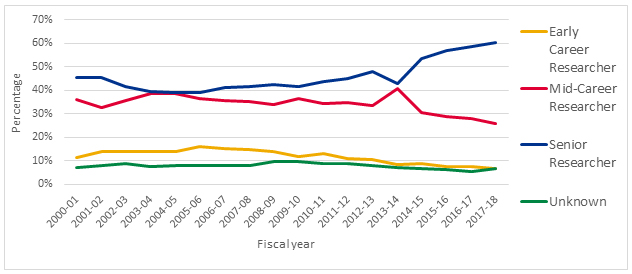
Figure 18 – Long Description
| Career Stage | 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Early Career Researcher | 12% | 14% | 14% | 14% | 14% | 16% | 15% | 15% | 14% | 12% | 13% | 11% | 11% | 9% | 9% | 8% | |
| Mid-Career Researcher | 36% | 33% | 36% | 39% | 39% | 36% | 36% | 35% | 34% | 37% | 34% | 35% | 33% | 41% | 31% | 29% | |
| Senior Researcher | 45% | 45% | 42% | 40% | 39% | 39% | 41% | 42% | 42% | 42% | 44% | 45% | 48% | 43% | 53% | 57% | |
| Unknown | 7% | 8% | 9% | 8% | 8% | 8% | 8% | 8% | 10% | 10% | 9% | 9% | 8% | 7% | 7% | 6% |
Figure 18: Leverage Ratio of Partnerships: Partners to Investments out of IA’s ISI Budget
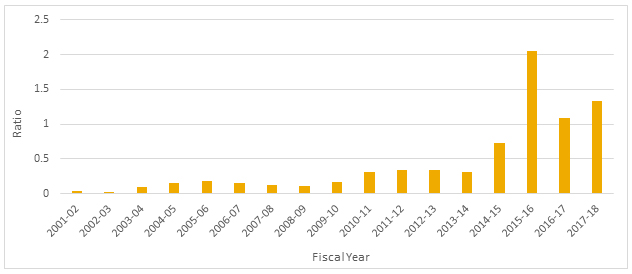
Figure 18 – Long Description
| 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Leverage ratio | 0.034737661 | 0.023481962 | 0.095878106 | 0.152317781 | 0.18590395 | 0.151402168 | 0.117817623 | 0.108454327 | 0.165348825 | 0.310075882 | 0.343017378 | 0.340344013 | 0.310106015 | 0.730849706 | 2.047299505 | 1.082459282 | 1.331611198 |
Figure 19: Leverage Ratio of Partnerships: Partnership Contributions and IA’s ISI Budget
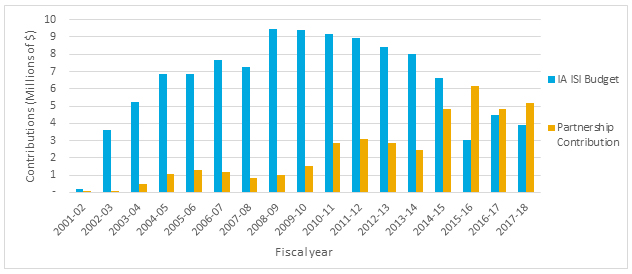
Figure 19 – Long Description
| 2001-2002 | 2002-2003 | 2003-2004 | 2004-2005 | 2005-2006 | 2006-2007 | 2007-2008 | 2008-2009 | 2009-2010 | 2010-2011 | 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IA ISI Budget | $ 179,920.00 | $ 3,594,950.84 | $ 5,251,047.62 | $ 6,862,980.76 | $ 6,854,087.82 | $ 7,669,434.45 | $ 7,274,972.80 | $ 9,445,238.60 | $ 9,378,935.71 | $ 9,144,510.00 | $ 8,944,293.11 | $ 8,432,944.00 | $ 7,997,049.00 | $ 6,605,118.62 | $ 3,021,131.00 | $ 4,466,653.00 | $ 3,877,566.52 |
| Partnership Contribution | $ 6,250.00 | $ 84,416.50 | $ 503,460.50 | $ 1,045,354.00 | $ 1,274,202.00 | $ 1,161,169.00 | $ 857,120.00 | $ 1,024,377.00 | $ 1,550,796.00 | $ 2,835,492.00 | $ 3,068,047.97 | $ 2,870,102.00 | $ 2,479,933.00 | $ 4,827,349.00 | $ 6,185,160.00 | $ 4,834,970.00 | $ 5,163,411.00 |
Figure 20: ISG Funding
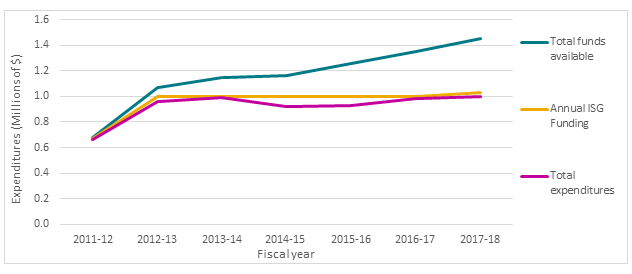
Figure 20 – Long Description
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|
| Total funds available | $ 674,542 | $ 1,073,019 | $ 1,146,515 | $ 1,161,990 | $ 1,256,478 | $ 1,349,436 | $ 1,448,910 |
| Annual ISG Funding | $ 666,667 | $ 1,000,000 | $ 1,000,000 | $ 1,000,000 | $ 1,000,000 | $ 1,000,000 | $ 1,030,000 |
| Total expenditures | $ 664,178 | $ 959,635 | $ 988,203 | $ 919,028 | $ 930,429 | $ 985,219 | $ 1,002,348 |
Figure 21: Percentage of the Utilization of ISG Funds
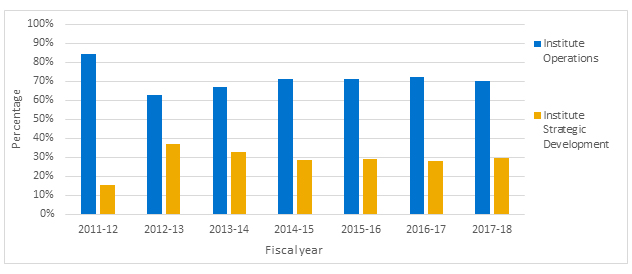
Figure 21 – Long Description
| 2011-2012 | 2012-2013 | 2013-2014 | 2014-2015 | 2015-2016 | 2016-2017 | 2017-2018 | |
|---|---|---|---|---|---|---|---|
| Institute Operations | 84% | 63% | 67% | 71% | 71% | 72% | 70% |
| Institute Strategic Development | 16% | 37% | 33% | 29% | 29% | 28% | 30% |
Figure 22: Institute Strategic Development Expenditures 2011-12 to 2017-18
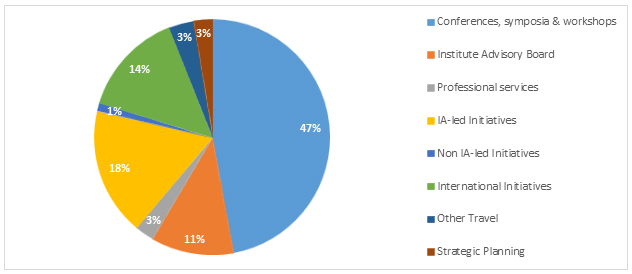
Figure 22 – Long Description
| Conferences, symposia & workshops | 47% |
|---|---|
| Institute Advisory Board | 11% |
| Professional servicess | 3% |
| IA-led Initiatives | 17% |
| Non IA-led Initiatives | 1% |
| International Initiatives | 14% |
| Other Travel | 3% |
| Strategic Planning | 3% |
Appendix 4: Sample list of Partners
- Canadian Digestive Health Foundation
- Alzheimer Society of Canada
- Alzheimer Society of Saskatchewan
- Ovarian Cancer Canada (Toronto)
- BC Cancer Agency (Vancouver, BC)
- CancerCare Manitoba
- Canadian Nurses Foundation (Ontario)
- Ontario Ministry of Health
- Natural Sciences and Engineering Research Council of Canada (NSERC)
- Nova Scotia Health Research Foundation
- British Columbia Ministry of Health (Victoria)
- Canadian Foundation for Healthcare Improvement (Ottawa)
- The CAPITAL CARE Group (Edmonton)
- Canadian Occupational Therapy Foundation
- AstraZeneca Canada Inc.
- Pfizer Canada Inc. (Quebec)
- Heart and Stroke Foundation of Canada (Ottawa, Ontario)
- St-Joseph's Health Care London - Parkwood Institute
- Heart and Stroke Foundation of Ontario (Toronto)
- National Natural Science Foundation of China (Haidian, Beijing)
- Japan Society for the Promotion of Science
- Veterans Affairs Canada
- Ontario Neurotrauma Foundation
- Physiotherapy Foundation of Canada
- The Academy of Finland
- Alberta Health Services
- Interior Health Authority (Kelowna, BC)
- Alberta Innovates Corporation
- Michael Smith Foundation for Health Research
- Rx&D Health Research Foundation
- The Foundation Fighting Blindness (Canada)
- Economic and Social Research Council (UK)
- Parkinson Society Canada (Toronto)
- Can. Assoc. Speech Language Pathologists (Toronto)
- The French National Research Agency (France)
- Fonds de recherche du Québec - Santé (FRQS)
- The Change Foundation
- Canadian Patient Safety Institute
- Canadian Physiotherapy Association (Ottawa, Ontario)
- The Swedish Council for Working Life and Social Research (Sweden)
- Israeli Ministry of Health
- Biotechnology and Biological Sciences Research Council (UK)
- National Research Fund (Luxembourg)
- Ste-Anne's Hospital Foundation (Quebec)
- Hotchkiss Brain Institute (University of Calgary)
- Deutsche Zentrum für Neurodegenerative Erkrankungen (Germany)
- Ministero della Salute (Italy)
- Medical Research Council (UK)
- Instituto de Salud Carloss III (Spain)
- Ottawa Hospital Research Institute
- University of Ottawa Heart Institute
- Hypertension Canada (Markham, Ontario)
- McGill University
- Libin Cardiovascular Institute of Alberta
- University of Alberta
- University of Western Ontario
- ThéCell : Le réseau de thérapie cellulaire et tissuaire du FQRS (Québec)
- Date modified: