Internal Assessment for 2011 International Review - CIHR Institute of Nutrition, Metabolism and Diabetes
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures and Tables
- Figure 1: 2008 INMD environmental scan results - respondent views on options for INMD to maintain or expand strategic priority beyond obesity and healthy body weight (N=645)
- Figure 2: Percentage of total CIHR expenditures in grants, salary awards and training awards related to the INMD mandate in open and strategic competitions between 2000–2001 and 2009–2010
- Figure 3: Fold increase from 2000 to 2010 in CIHR expenditures related to INMD mandate by theme, 2000–2001, 2005–2006 and 2009–2010
- Figure 4: Specialization index and average of relative citations for the top 10 countries publishing in obesity, 2000–2008
- Figure 5: CIHR open and strategic grant expenditures related to obesity and healthy body weight from 2000–2001 to 2009–2010
- Table 1: Total number of publications of top 10 countries in obesity, 2000–2008
Mandate and Context
Mandate
The Institute of Nutrition, Metabolism and Diabetes (INMD) is mandated to support research that enhances health in relation to diet, digestion, excretion and metabolism for a wide range of conditions and problems associated with hormone, digestive system, kidney and liver function.
Canada has a rich legacy in areas covered by the INMD mandate, most notably in the area of diabetes research. One of Canada's most recognized scientists, Dr. Fredrick Banting, along with Dr. John Macleod was awarded the Nobel Prize in Physiology or Medicine in 1923 for the discovery of insulin and its use in the treatment of type 1 diabetes. Today, many Canadian investigators are internationally recognized for their research in diabetes and the other INMD-mandate areas.
Structure and operations
Since 2009, INMD has been headed by Dr. Philip Sherman, an internationally-recognized leader in gastroenterology. Dr. Sherman is based at the Hospital for Sick Children and is supported by a small staff in Toronto and at CIHR headquarters in Ottawa. INMD receives strategic advice from its Institute Advisory Board (IAB), composed of leading researchers and partners drawn from across the spectrum of INMD's diverse communities and research disciplines. One of the key members of the IAB is the ethics designate, who provides advice to the board on ethics issues and represents INMD at teleconferences and annual meetings of the CIHR IAB Ethics Designates, coordinated by the CIHR Ethics Office.
The INMD niche
Over the past 10 years, INMD has forged a unique research agenda to address an emerging public health issue, obesity, which in 2004 affected almost one-quarter of the adult Canadian population.Footnote 1
INMD was created at a time of increasing awareness about the rising cost of obesity in Canada.Footnote 2 Many other developed countries had also identified obesity and overweight as a major public health issue.Footnote 3 Health authorities warned of the increased prevalence of obesity and overweight and its impact on chronic diseases.Footnote 4 After extensive consultation, the Institute's inaugural scientific director, Dr. Diane Finegood and the INMD IAB were compelled by the health research imperative posed by obesity and its consequences to identify obesity and healthy body weight (OHBW) as the single strategic focus of the Institute.
The choice of a single strategic priority – obesity and healthy body weight – distinguished INMD from the 12 other CIHR Institutes.
Responses to the 2006 CIHR International Review
While the choice of OHBW as INMD's single strategic priority was deemed appropriate by the 2006 CIHR International Review Panel, the same panel identified specific recommendations for improvement. The key recommendations are summarized below, with INMD's response to each.
2006 International Review recommendation related to the INMD single strategic priority
"INMD made a risky and far-sighted decision in choosing to concentrate their efforts on a single strategic priority. It is recommended that INMD and CIHR should carefully monitor the results of the implementation of this approach to determine its overall effectiveness."
In response to this recommendation from the review panel, in 2009 INMD commissioned a bibliometric study to measure the impact of the OHBW initiative and updated it for the 2011 International Review (see Outcomes and Outputs section). INMD also conducted an environmental scan in 2008 to gather researcher and stakeholder perspectives that would inform the Institute's future strategic priorities and directions.
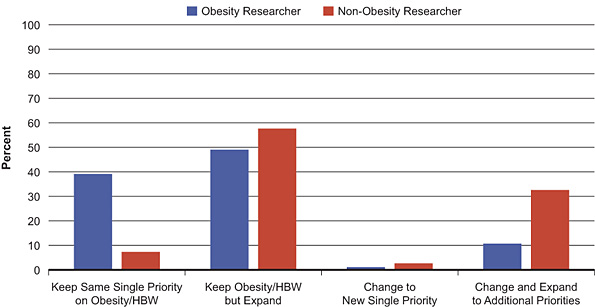
Figure 1 illustrates that the overwhelming majority of respondents to the 2008 environmental scan indicated that INMD should keep OHBW as a priority, but expand it to include other research priorities, regardless of whether the researcher had indicated their own primary research focus was obesity. This became an assumption going forward in updating INMD's strategic plan in 2009 (see Going Forward section).
Figure 1: 2008 INMD environmental scan results – respondent views on options for INMD to maintain or expand strategic priority beyond obesity and healthy body weight (N=645)
2006 International Review recommendation related to communications
"INMD should endeavour to reach out to the full range of researchers and stakeholders in its community, including, for example, researchers who may feel disenfranchised and those from fields such as social sciences that may not have traditionally done obesity-related research."
In January 2009, INMD established a monthly newsletter. This newsletter is a vehicle for INMD to communicate to its diverse research communities, and serves as a way to engage communities about INMD's mandate and promote the new strategic priorities. INMD has also reached out through extensive consultations with various research communities to develop a new strategic plan (see Going Forward section), and is nurturing partnerships with previously disenfranchised communities to address the increased breadth of the new INMD strategic plan.
The 2006 International Review also included recommendations for improvements in knowledge translation, contributing to the ethics mandate, and performance monitoring and reporting. This report highlights key activities undertaken in response to each of these recommendations.
Institute Priorities
The first INMD strategic plan was released in 2002. This plan was updated twice between 2002 and 2009. The most recent version of the strategic plan, which covers the period 2010–2014, is described in the Going Forward section of this report.
In September 2001, INMD initiated an environmental scan of its stakeholders and potential partners. The consultation was called Charting Our Course. Obesity and healthy body weight (OHBW) emerged as a single research priority for advancing knowledge and building capacity.
Between 2000 and 2005, INMD worked in collaboration with many partners, including the Heart and Stroke Foundation of Canada (HSFC), the Canadian Diabetes Association (CDA), other CIHR Institutes and Obesity Canada (a non-profit organization), to organize workshops and launch funding opportunities related to OHBW.
In 2005, a new obesity research funding leader in Canada emerged. The HSFC prioritized obesity research and became INMD's closest collaborator on OHBW initiatives. Then the Canadian Obesity Network (CON) was created to act as a catalyst for addressing obesity in Canada. The CON remains a valuable partner to INMD, particularly in relation to knowledge translation (KT).
Internationally, childhood obesity has emerged as an important research issue.Footnote 5 The Government of Canada released the Integrated Pan-Canadian Healthy Living Strategy in 2007 and several provinces, including British Columbia and Ontario, funded strategies to promote healthy body weights that had a focused component on children. As these strategies were developed, a dearth of evidence was recognized on best practices and policies for addressing OHBW at the population level. This provided the impetus for INMD to champion intervention research in collaboration with the CIHR Institute of Population and Public Health (IPPH).
Key Initiatives
Over the past 10 years, INMD has launched a variety of strategic funding initiatives to advance knowledge, build researcher capacity and support knowledge translation in the area of obesity and healthy body weight (OHBW). These initiatives demonstrate the transformative effect of INMD in OHBW, illustrate the beneficial impact of targeted research and highlight the Institute's ability to collaborate with partners to address a public health priority. In total, INMD invested ~$34M in OHBW research over the 10 years up to 2009–2010, which represents ~62% of the INMD strategic budget.
INMD's focus on a single strategic priority did not mean that the Institute provided exclusive funding and support to obesity.
INMD also pursued opportunities in partnership with stakeholders in other areas of the mandate, such as nephrology, digestive diseases and diabetes. Two targeted initiatives highlighted in this report are ones that INMD launched with partners to meet specific objectives in nephrology and gastroenterology.
Initiative 1: Obesity and healthy body weight –INMD's flagship initiative
Advancing knowledge and building capacity through targeted research
INMD launched a portfolio of complementary funding opportunities under the OHBW initiative. INMD funded the development of new ideas by supporting 32 pilot projects and eight planning development grants, and built research capacity through funding 10 training awards for fellows, doctoral research students, and new investigators, and one Strategic Training Initiative in Health Research (STIHR) grant that was renewed in 2009 for six years.
INMD also facilitated multidisciplinary team-based research by funding 10 New Emerging Teams and four Emerging Team Grants, and supported highly-ranked obesity grant applications that were not funded in the CIHR Open Operating Grants competition through Obesity Bridge Grants in all areas of the CIHR research mandate (N=33). In addition, INMD supported research and knowledge translation in four childhood obesity competitions for a total of 18 grants, 28 Intervention Research Operating Grants, seven Obesity and Built Environment Grants, three Partnerships for Health System Improvement Grants, and 22 Meeting, Planning and Dissemination grants.
Between 2000 and 2010, OHBW became a major focus of Canadian public health authorities at the federal, provincial/territorial and regional/municipal levels. As a result, three CIHR institutes and six external organizations have partnered with INMD to support OHBW research.
Knowledge translation
INMD demonstrated national leadership in determining OHBW research priorities by convening a national meeting in 2005 entitled Addressing Obesity in Canada – A Think Tank on Selected Policy Research Priorities. Six organizations, representing research funders, government and non-governmental organizations, collaborated in this think tank which aimed to identify key policy questions that could be informed through a targeted research agenda. This integrated approach to knowledge translation resulted in the launch of an obesity and built-environment research initiative.
INMD's targeted funding, Intervention Research – Healthy Living and Chronic Disease Prevention, resulted from INMD's involvement in developing the Integrated Pan-Canadian Healthy Living Strategy.Footnote 6 INMD and partners have funded 30 intervention research projects since 2006. The objectives of this funding mechanism were to support research on rapidly unfolding natural experiments that address chronic disease prevention at the population level, encourage innovative research in collaboration with community, non-profit, private and public partners, and develop bidirectional knowledge exchange opportunities.
Sustaining the research pipeline across the INMD mandate
In 2005, to better support a rigorous and competitive pipeline across the mandate, INMD launched bridge grants. Bridge grants support highly-rated grant applications submitted to the CIHR Open Operating Grant competition that fall just below the overall funding cut-off. Each grant provides up to $100,000 for one year. INMD funded 62 bridge grants between 2005 and 2010 ($5.5 million).
In 2010, INMD surveyed recipients of bridge grants to determine the program's impact. Of the 34 respondents (68% response rate), the majority (n=28) indicated that they could not have sustained the momentum for their research projects in the absence of INMD one-year bridge funding. They also indicated that bridge funding helped them secure a subsequent CIHR Operating Grant. Other benefits researchers noted were that bridge funding enabled them to maintain momentum in research projects and publications, retain trainees and highly qualified technical personnel, maintain advancements in the field and preserve expertise that would have jeopardized the feasibility of their research program had it been lost.
In 2009, INMD shifted the focus of bridge grants to support researchers who either are not currently funded or hold just one CIHR grant for which they are applying for a renewal, and to new investigators, assistant professors and clinician-researchers. This change is intended to enhance support along the early career trajectory.
Initiative 2: Capacity building in nephrology – KRESCENT
The Kidney Research Scientist Core Education and National Training Program (KRESCENT) is a funding and mentoring program for doctoral students, postdoctoral fellows and new investigators who are interested in research activities related to kidney health and disease. This initiative is a joint effort of the Kidney Foundation of Canada (KFOC), the Canadian Society of Nephrology (CSN), INMD, the Institute of Circulatory and Respiratory Health (ICRH) and industry. The program was first launched in 2004 and continues today.
The goal of the KRESCENT program is to establish a new generation of kidney scientists with greater ability and opportunity to perform transdisciplinary research. This approach is reflected in funding, which was equally divided among MD and PhD students. Of the 17 trainees who completed the fellowship stage of KRESCENT, 15 have secured academic appointments. Approximately half of the trainees have already secured extramural grant support for their independent research activities.Footnote 7
Initiative 3: Capacity building – Gastroenterology
CIHR and INMD have two longstanding research funding partnerships with the gastroenterology community: the Canadian Association of Gastroenterology (CAG) and the Canadian Digestive Health Foundation (CDHF). Both programs focus on capacity building.
The CIHR-CAG funding competition has become the premier capacity-building initiative for gastrointestinal research in Canada. It facilitates clinical and translational research. Since its inception, multiple industry partners have participated, such as AstraZeneca Canada, Abbott, Ferring, Shire Limited, Olympus, the Institute of Infection and Immunity, and the Crohn's and Colitis Foundation of Canada.
More than $11 million dollars has been awarded over 15 years. Funding was leveraged 1:1 for awards and 2:1 (Industry-CIHR) for operating grants. Almost $9 million of the $11 million was dedicated to training awards, which have provided support for 78 fellowship and new investigator awards, 28% for MD students and 72% for PhD students.
The CDHF partnership focuses on funding postdoctoral-level students and complements the CAG funding programs. Since 2001, the co-funded CDHF and CIHR program has provided more than $1 million to fund 29 post-doctoral students at 12 universities across Canada.
Ethics and partnerships
In an initiative to address childhood obesity called Building Trust, INMD has played a leadership role in exploring ethical issues related to partnerships among the private sector, researchers and government. Two meetings, one in 2005 and a subsequent meeting in 2009, brought together 50 national and international leaders from industry, non-governmental organizations, research and government. The goal was to create an environment in which the four sectors could better communicate and engage and, as a result, enable greater cooperation and ethical partnerships between the food industry and the health sector. INMD continues to advance work towards greater intersectoral collaboration, as evidenced by the January 2010 workshop, Developing a Research Agenda to Support Sodium Reduction in Canada (see Informing decision making in Outputs and Outcomes section).
Institute funding
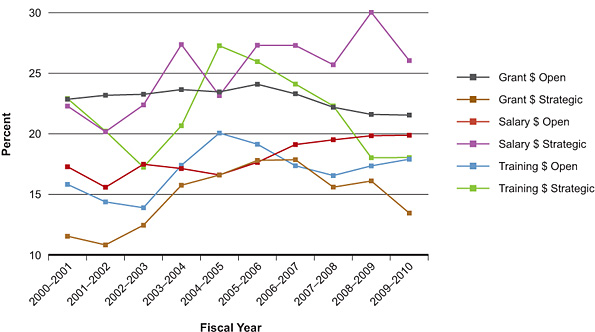
Success in the investigator-driven open competitions can be used to indicate the strength of a research community. As shown in Figure 2, expenditures for INMD-related research represent a sizeable portion of CIHR's total open grants, salary awards and training awards. INMD-related open grant expenditures have increased 1.8-fold, representing 22.9% ($56.5 million) and 21.5% ($100.9 million) of CIHR's total open grant expenditures in 2000–2001 and 2009–2010, respectively. Within these open grant expenditures, all INMD mandate area expenditures increased. The increases in the open grants in INMD mandate areas from 2000–2001 to 2009–2010 were 2.4-fold for diabetes; 1.2-fold for endocrinology; 2.2-fold for gastroenterology; 2.2-fold for kidney; 1.5-fold for liver; 1.9-fold for metabolism; 2.4-fold for nutrition and 5.7-fold for obesity.
While fluctuations occur between individual years, over the entire period open salary awards and open training awards have increased as a proportion of CIHR's total expenditures in these categories. INMD-related open salary awards increased from 17.3% ($4.4 million) to 19.9% ($3.7 million), while INMD-related open training awards increased from 15.8% ($4.7 million) to 17.9% ($9.5 million) between 2000–2001 and 2009–2010, respectively. It is important to note that expenditure fluctuations shown in Figure 2 in the open salary award category relate directly to the overall CIHR budget. For instance, while actual expenditures of open salary awards have decreased, they have not decreased as dramatically as CIHR's total expenditures in open salary awards. The INMD-related proportional increase indicates that INMD-related salary awards are receiving a greater portion of CIHR's decreased expenditures for open salary awards. This demonstrates the strength of award holders in INMD-related areas.
Figure 2: Percentage of total CIHR expenditures in grants, salary awards and training awards related to the INMD mandate in open and strategic competitions between 2000–2001 and 2009–2010.
With respect to strategic funding, INMD-related strategic grant expenditures increased 9.2-fold between 2000–2001 ($3.5 million) and 2009–2010 ($32.1 million). Proportional to CIHR's total strategic grant expenditures, INMD-related strategic grant expenditures fluctuate over time. A decrease in proportional expenditures in recent years may be due to the completion of high-value grants (e.g., STIHRs) related to INMD research areas.
INMD-related strategic salary award expenditures increased 3.6-fold between 2000–2001 ($0.8 million) and 2009–2010 ($3 million) and strategic training award expenditures increased 4.5-fold ($0.7 million in 2000–2001 to $3.2 million in 2009–2010). Fluctuations occur between individual years. However, over the entire period, strategic salary awards have increased as a proportion of CIHR's total strategic salary awards (22% in 2000–2001 to 26% in 2009–2010). While strategic training award expenditures have increased over time, this growth has not kept pace with CIHR's total strategic training award growth, in part due to the introduction of the Canada Graduate Scholarships Program in 2003–2004. INMD-related strategic training awards represented 22.9% and 18.0% of CIHR's total expenditures in 2000–2001 and 2009–2010, respectively.
Taken together, these data show that INMD-related funding represents a sizeable proportion of the total CIHR funding allocated in open and strategic grant competitions. These data are subject to limitations; findings are based on a keyword search of the CIHR funding database that was then validated through a subjective process. Multiple institute affiliations are possible for any project. Note that the term "strategic funding" includes funding from the INMD strategic initiatives budget as well as strategic funding from other CIHR sources, such as knowledge translation partnerships and ethics.
Figure 3 illustrates INMD-related expenditures by the four CIHR-mandated themes that the grant holders voluntarily assigned to their projects. It indicates that INMD-related health services research and population and public health research funding have increased dramatically compared to biomedical and clinical research. These findings are subject to limitations because they are based on voluntary assignment, not validated by staff and many grant holders did not assign a theme to their research proposal.
Figure 3: Fold increase from 2000 to 2010 in CIHR expenditures related to INMD mandate by theme, 2000–2001, 2005–2006 and 2009–2010
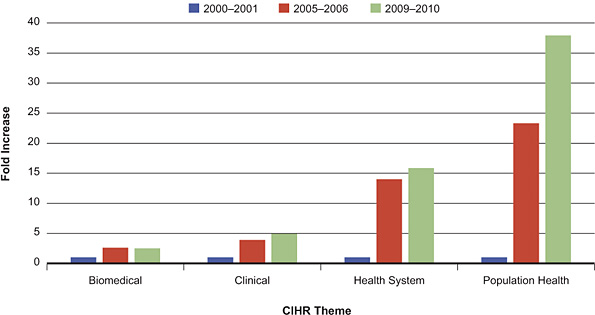
INMD-related expenditures remained highest in biomedical research at $97.8 million in 2009–2010, representing a 2.5-fold increase over 10 years. INMD-related expenditures in clinical research were $25.7 million in 2009–2010, which represents a five-fold increase. INMD-related expenditures in health services research were $4.4 million in 2009–2010, which represents a 16-fold increase over 10 years. INMD-related expenditures in population and public health research increased 38-fold over 10 years to $18.4 million in 2009–2010. (These data are subject to limitations. Identification of research theme is researcher selected, selection is not validated and a high proportion of researchers did not select a research theme in the early years.)
Outputs and Outcomes
In preparation for the 2011 CIHR International Review, INMD worked with the CIHR Impact Assessment Unit to conduct a bibliometric study of obesity. This study was conducted by the Observatoire des sciences et des technologies using Thomson Reuters' Web of Science and was completed in July 2010. Given that Thomson's databases do not have a subject classification for individual papers, the U.S. National Library of Medicine Medical Subject Headings (MeSH) term "obesity" was used to retrieve papers in the PubMed database on obesity over the 1997–2008 period. In addition to the papers retrieved using MeSH headings, papers published in core journals of obesity were systematically included in the dataset. Databases searched may not cover all publications in this area and average of relative citations (ARC) data are incomplete for 2008. Countries were ranked based on total number of publications over the time period.
Advancing knowledge
Obesity research in Canada – A CIHR success story
One of the measures of knowledge creation is the number of peer reviewed research publications in a subject area. Table 1 shows that Canada ranked fifth in the world for total number of publications in obesity between 2000 and 2008. Between 2000 and 2008, the annual number of Canadian obesity research publications tripled, from 93 in 2000 to 283 in 2008.
Table 1: Total number of publications of top 10 countries in obesity, 2000–2008
| United States | 14,830 |
| United Kingdom | 2,930 |
| Italy | 1,762 |
| France | 1,609 |
| Canada | 1,588 |
| Germany | 1,565 |
| Japan | 1,535 |
| Australia | 1,441 |
| Sweden | 1,185 |
| Spain | 1,126 |
Source: Observatoire des sciences et des technologies (Thomson Reuters' SCI Expanded, SSCI & AHCI) – Current as of July 2010
Figure 4 illustrates the specialization index (SI) and ARC in obesity publications for the top 10 countries. When the SI is greater than one, it indicates that the country of interest is more specialized in its priority area, compared to the world average. Similarly, an ARC >1, means the papers are cited more frequently than the world average in its priority area.
Figure 4: Specialization index and average of relative citations for the top 10 countries publishing in obesity, 2000–2008
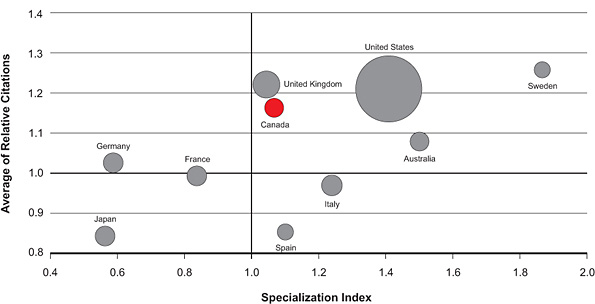
Canada scores above the world average in obesity publications for both the SI and the ARC. Canada ranks fourth for ARC (1.16) and fifth for SI (1.06) in obesity among the top 10 countries for the period 2000–2008. The size of the circle in the figure illustrates the number of publications in the area from 2000–2008.
Selected examples of influential Canadian obesity publications published by CIHR-funded researchers that were frequently cited and published in high impact journals from 2000–2008:
-
Yusuf, Hawken, Ounpuu, et al. published Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries, in Lancet in 2004 (1,306 citations).
-
Després, Golay and Sjostrom published Effects of rimonabant on metabolic risk factors in overweight patients with dyslipidemia in the New England Journal of Medicine in 2005 (803 citations).
-
Yusuf, Hawken, Ounpuu, et al. published Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study, in Lancet in 2005 (492 citations).
-
Lewis, Carpentier, Adeli and Giacca published Disordered fat storage and mobilization in the pathogenesis of insulin resistance and type 2 diabetes in Endocrine Reviews in 2002 (349 citations).
-
Després and Lemieux published Abdominal obesity and metabolic syndrome in Nature in 2006 (395 citations).
Commenting on the impact of his work, Salim Yusuf of McMaster University stated: "The INTERHEART StudyFootnote 8 demonstrated that more than 90% of the risk of myocardial infarction worldwide in both sexes and at all ages can be attributed to nine risk factors: abnormal lipids, smoking, hypertension, diabetes, abdominal obesity, psychosocial factors, consumption of fruits and vegetables, alcohol, and regular physical activity. This study was supported by CIHR in collaboration with other funders and demonstrates the impact of Canadian researchers in global research efforts to reduce the burden of chronic disease."
Could INMD have been responsible for these increases? Although the increase in the number of Canadian obesity-related publications and the ARC correspond temporally to the time period when INMD launched the obesity and healthy body weight (OHBW) initiative, the search methodology does not permit an accurate attribution by institute.
Internal indicators of success
An analysis of files retrieved from an unvalidated keyword search for the terms "obesity", "healthy weight" and "body weight" in the titles of grant applications submitted to CIHR shows an 8.4-fold increase in the total number of obesity-related applications reviewed between 2000–2001 and 2009–2010. A comparable review of validated funded grant data suggests an underestimation of the total number of obesity-related applications. Thus, the 8.4-fold increase gives an indication of the minimum magnitude of increased application pressure.
In response to the growing number of obesity-related grant applications submitted to CIHR in the Open Operating Grant Program, CIHR revised the mandate of one of the peer review committees. The new committee, Diabetes, Obesity, Lipid & Lipoprotein Disorders (DOL), has a mandate to review applications related to "Molecular, cellular and whole organism studies of carbohydrate, lipid and energy metabolism as related to both fundamental and translational biology of diabetes, obesity, insulin resistance and dyslipidemia." Previously, this grant-review panel was more focused on metabolism.
The establishment of the Diabetes, Obesity, Lipid & Lipoprotein Disorders committee reflects an increase in application pressure, and indicates that the cadre of Canadian obesity researchers has grown and is highly competitive.
External indicators of success
In April 2010, Science Watch, a group that tracks trends and performance in basic research, ranked Université Laval and the University of Toronto in the top 20 institutions by number of papers published on obesity between 1999 and 2009.Footnote 9
Impact across the INMD mandate
Canadian investigators in the INMD mandate area excel in the creation of new knowledge that meets international standards of scientific excellence. The following are some examples.
Diabetes
"Almost every international diabetes congress, society, journal and funding agency consistently and prominently features Canadian researchers in diabetes leadership roles. Either directly or through extensive collaborative networks, Canadian researchers are actively establishing new frontiers, methodologies and directions. Because diabetes affects many systems and disciplines, such collaborations span the whole range of biologic and clinical research. For example, the Canadian-led international Diabetes REduction Assessment with Ramipril and Rosiglitazone Medication (DREAM) trial of more than 5,000 people with pre-diabetes was the largest diabetes prevention trial ever conducted.Footnote 10 Funded by CIHR and a consortium of three companies, this trial showed that ramipril may promote regression to normal glucose levels and that rosiglitazone dramatically prevented diabetes."
Advances in lipoprotein metabolism
"Canadian investigators published the first studyFootnote 11 that established a strong link between the gut hormone, Glucagon-Like Peptide-2 (GLP-2), and intestinal fat absorption and chylomicron production. GLP-2 stimulates rapid dietary fat absorption and increases postprandial lipid excursion via stimulation of CD36. These findings implicate GLP-2 as a nutrient-dependent signal that regulates intestinal lipid absorption and the assembly and secretion of triglyceride-rich lipoproteins from intestinal enterocytes."
Gastroenterology – Translating basic discoveries to improved patient care
"The Montreal ClassificationFootnote 12 (MC) was a pioneering attempt at moving the classification of inflammatory bowel disease (IBD) from clinical descriptors to genetic and serological descriptors that take into account disease etiology. The MC is now in regular use by most studies that publish genotype-phenotype studies in IBD. As new genetic and other molecular markers continue to be discovered, I look forward to seeing these integrated into future revisions of the MC, so the day will arrive when we no longer use the terms Crohn's disease and ulcerative colitis but, rather, for example: NOD2+/ASCA+IBD."
Hepatology
"Funds awarded by CIHR over the years have been pivotal in supporting new breakthroughs in the understanding of chronic liver diseases, including the discovery of genes predisposing to the chronic autoimmune illness, Primary Biliary Cirrhosis.Footnote 13"
Capacity building
Obesity and healthy body weight
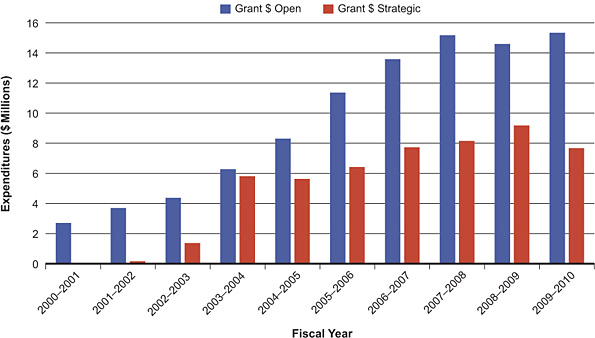
In all of INMD's strategic funding initiatives related to OHBW, capacity building was a key component. The increased number of CIHR OHBW-related grants awarded in open and strategic competitions between 2000–2001 (31 and 2, respectively) and 2009–2010 (134 and 103, respectively) provides evidence of enhanced capacity. Figure 5 shows increased levels of CIHR funding related to OHBW in the open and strategic competitions, from 2000–2001 to 2009–2010. The increase in open grant expenditures reflects the increase in highly competitive capacity in obesity.
Figure 5: CIHR open and strategic grant expenditures related to obesity and healthy body weight from 2000–2001 to 2009–2010
INMD-supported training to build capacity in obesity research
The CIHR-funded Strategic Training Initiative in Health Research (STIHR), Training Program in Obesity/Healthy Body Weight Research was launched in 2003 at Université Laval. The goal of this training grant was to consolidate, develop and implement a distinctive program to train the next generation of Canadian researchers in obesity.
The training program, led by Dr. Denis Richard, Director of the Hôpital Laval Research Centre and the Merck Frosst/CIHR Research Chair in Obesity, has supported 19 MSc, 19 PhD and 14 postdoctoral fellows through studentships and scholarships. These students and postdoctoral fellows have contributed to 163 peer-reviewed articles and more than 170 scientific communications. The majority of the graduates are pursuing further research training or work in research-related fields.
The STIHR also supports the Summer Obesity Boot Camp, which was established in 2006 and is co-led by the Canadian Obesity Network (CON) (a Network of Centres of Excellence), Université Laval and the University of Alberta. This retreat transfers research findings and builds a sense of community for the top young students and professionals working in obesity. Students spend nine days learning and networking with 13 established Canadian obesity researchers. To date, 125 trainees have completed the boot camp.
The next generation of obesity and chronic disease researchers
INMD's funding of new emerging teams and Emerging Team Grants are other examples of capacity building. In 2010, INMD conducted an online survey of these grant recipients. Seven of 18 funded teams participated in the survey, with the following synopsis:
-
Over eight years, the seven teams report training 15 new investigators, 21 postdoctoral fellows and 33 doctoral students.
-
Four teams recruited international students.
-
Five teams noted that their grant supported formal qualifications (e.g. PhD) for project members.
One survey respondent stated that the team grant "allowed our institution to form a high-level, coordinated, transdisciplinary researchs team, which has created a platform for collaborative research amongst previously isolated investigators, and it has attracted many new collaborators from outside of the institution."
Nephrology
Indicators show that the KRESCENT program has been successful in enhancing kidney research capacity in Canada. One KRESCENT trainee, Michael Walsh at McMaster University, participated in an international study, Rituximab versus Cyclophosphamide in ANCA-Associated Renal Vasculitis, which was recently published in the New England Journal of Medicine.Footnote 14 Another former KRESCENT trainee recently published in the highest impact kidney journal, Journal of the American Society of Nephrology. Dr. Nina Jones, now a principal investigator at the University of Guelph, is first author on a 2009 publication that demonstrates that the phosphotyrosine-binding adaptor protein Nck is essential for podocyte function.Footnote 15
Informing decision making
Informing government decision making
Both INMD scientific directors have appeared before the Canadian House of Common's Standing Committee on Health to provide science advice on issues relevant to the INMD mandate, including childhood obesity,Footnote 16 food labeling and sodium reduction, demonstrating INMD's relevance to policy makers. INMD is informing decision making, which is an essential part of the CIHR mandate related to knowledge translation.
Sodium reduction in Canada
The Sodium Reduction Strategy for Canada was released in July 2010. Research is one of three components of the strategy, and INMD played a leadership role in developing the research agenda to support sodium reduction in Canada. In January 2010, INMD co-hosted a workshop with the CIHR Institute of Circulatory and Respiratory Health (ICRH) called Developing a Research Agenda to Support Sodium Reduction in Canada. The workshop engaged the Institute of Population and Public Health (IPPH) and the Institute of Human Development, Child and Youth Health (IHDCYH), as well as external partners Health Canada, Public Health Agency of Canada, Blood Pressure Canada, Canadian Stroke Network, the Advanced Food and Materials Network and HSFC. The outcomes of this workshop provided the content for the research component of the Sodium Reduction Strategy for Canada.
To address research gaps identified at the workshop, INMD has twice launched Sodium and Health funding opportunities. The first competition focused on basic research, and the second competition includes support for population health research related to sodium reduction, with ICRH, IHDCYH, IPPH and the Canadian Stroke Network included as partners. INMD has also been working with the Natural Sciences and Engineering Research Council to develop means to stimulate research related to food science and health to support technological innovations related to lowering sodium.Footnote 17 In addition, INMD is contributing to global efforts in this area by supporting an upcoming hypertension control initiative being launched through the Global Alliance on Chronic Disease, and by playing a key role in a recent World Health Organization meeting hosted in Canada to address sodium monitoring and surveillance at the population level.
Intervention research
INMD's targeted funding, Intervention Research – Healthy Living and Chronic Disease Prevention, was launched in 2006 with IPPH. IPPH now leads this initiative and INMD continues to be a key collaborator. In 2010, INMD and IPPH commissioned an independent evaluation to measure the impact of this initiative.
The evaluation provides evidence that this intervention research funding tool facilitates knowledge exchange and knowledge translation between researchers and decision makers. Two case studies highlighted in the evaluation address student health: Action Schools! British Columbia and the Support Healthy Living for Youth in Schools in Quebec. The evaluation found that government decision makers used the research results of these funded intervention research projects to validate their approach to school health. The Robert Wood Johnson Foundation in the United States has modeled its intervention research funding mechanism on this work.
Health and health system/care impacts
Clinical practice guidelines
Obesity Canada convened a panel of experts, which included the scientific director of INMD, to develop a comprehensive set of clinical practice guidelines that would address the management and prevention of obesity in adults and children.Footnote 18 There is continued commitment to improving clinical practice related to obesity as evidenced by INMD and CON co-hosting a bariatric care workshop in December 2010.
A survey of investigators holding INMD team grants was undertaken in 2010, and provides another example of the impact of a funded research team on health care. One of the funded teams evaluated the association between metformin and clinical outcomes in patients with heart failure and type 2 diabetes. Using a provincial health database, the investigators found that metformin, used alone or in combination in subjects with heart failure and type 2 diabetes, is associated with lower morbidity and mortality compared with alternative sulfonylurea monotherapy.Footnote 19 This finding resulted in a change in the drug monograph and the labeling of metformin to remove heart failure as a contraindication. As such, it has significant implications for patient care.Footnote 20 It was cited in the 2008 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada.Footnote 21
INMD has also played a supporting role in the development of clinical practice guidelines in gastroenterology. Paul Sinclair, CAG's executive director notes: "INMD contributed funding to five important clinical practice guidelines in gastroenterology-related health and disease, which are transforming practice, saving money and will ultimately improve the health of Canadians."Footnote 22,Footnote 23,Footnote 24,Footnote 25
Alan Barkun of McGill University states: "The recently published international recommendations on the management of patients with non-variceal upper gastrointestinal bleeding combined state-of-the-art guidelines development methodology and broad clinical input from recognized experts worldwide.Footnote 26 The support received from CIHR early in the process strengthened the credibility and validity of the effort, and was instrumental in allowing the multi-specialty society group to proceed and complete this important work. This is a great example of knowledge translation – bringing research to the bedside to improve patient care."
Transformative effects of the Institute
INMD's transformative effects are evident on the Canadian obesity research landscape.
Canadian obesity investigators ranked fifth in the world in terms of productivity between 2000–2008. During this time, research capacity also was built in Canada, as evidenced by the increase in obesity applications to the CIHR Open Operating Grant Program and the need for a new peer review committee. Canadian researchers advanced knowledge in the field at the international level, as demonstrated by high impact, widely-cited publications.
INMD also played a role in facilitating knowledge translation by supporting the development of clinical practice guidelines, as well as stimulating intervention research to study natural experiments that impact on OHBW.
In 2001, INMD set out to make obesity a national priority for the public, industry and government. Canadian news coverage of obesity has been prominent; for instance, in 2005–2006 media profile was logged at 5.9 million impressions.
INMD has played a key role in contributing to CIHR's overall vision and mandate. As a result of the expanded mandate, there have been funding increases in both population health and health services research across CIHR. INMD has played a key role in supporting OHBW research in these areas.
Important contributions to date are that INMD has:
-
enabled a small research community to become internationally recognized, independent and fundable in CIHR open research funding competitions, as evidenced by the creation of an obesity peer-review committee at CIHR and the almost six-fold increase in obesity funding in the open grants competition between 2000–2001 and 2009–2010
-
stimulated other research funders to choose obesity as a key research priority, including ICRH and IHDCYH and the Heart and Stroke Foundation of Canada
-
increased obesity research capacity by launching many competitions over the past 10 years that have led to a larger and more diverse research community, exemplified by increased funding applications at CIHR
-
demonstrated that CIHR can deliver on important government issues in a timely fashion, illustrated by intervention research
Going Forward
INMD strategic plan 2010–2014
Under the leadership of a new scientific director, INMD embarked on a strategic planning process in 2009 that was based on extensive consultation with various stakeholder communities. The assumption going forward in updating the INMD strategic plan was that INMD should keep OHBW as a priority and expand to include other relevant research priorities. This decision was taken as a result of the 2008 environmental scan so as to engage potentially disenfranchised research communities (as recommended in the 2006 International Review).
Engaging the full spectrum of stakeholders across the INMD mandate was recognized as one of the greatest challenges in going forward.
In 2009, the INMD team consulted more than 200 stakeholders (including researchers, government representatives and voluntary health organizations) in seven INMD strategic planning summits. During these summits, the need was emphasized for INMD to align its new strategic plan with CIHR's strategic plan for 2009–2010 to 2013–2014 (Health Research Roadmap: Creating Innovative Research for Better Health and Health Care). The principles and the process are described in detail in the INMD strategic plan for 2010–2014.Footnote 27
The INMD Institute Advisory Board (IAB) met in November 2009 to consider the wide-ranging input received from stakeholders and then determined the new INMD strategic priorities. The IAB considered input received from multiple sources in relation to criteria developed for decision making.
The IAB identified foundational principles that the new strategic research priorities were built on, including research excellence through partnerships, ethics, capacity, knowledge translation and evaluation. The four new strategic priorities of INMD are presented below. Note that the order of presentation does not imply a hierarchy of importance.
Food and health
INMD aims to develop a stronger evidence base to inform future nutritional practice and food policy. The Institute will foster research on the total diet and specific nutrients to enhance health and reduce the risk of chronic disease. This includes evaluating biomarkers of nutritional adequacy, emerging innovations in food engineering and the ethical issues posed by these changes, particularly with respect to people with vulnerabilities.
This work includes advancing knowledge in the following:
-
basic physiology, metabolism and homeostatic mechanisms (e.g., lymphatic growth response to salt intake, lipid droplet formation)
-
clinical research related to food and nutrition, nutrient requirements and maintenance
of health (e.g., micronutrient interventional research) -
food and nutrition policy research at the population level (e.g., sodium reduction, food fortification, functional foods, food security)
This Institute priority supports research priorities outlined in CIHR's overall strategic plan, Roadmap, related to promoting health and reducing the burden of chronic disease, and reducing health inequities of Aboriginal peoples and other vulnerable populations. It also links to initiatives that other CIHR institutes are undertaking – for example, personalized medicine (cancer research), epigenetics (Institute of Neurosciences, Mental Health and Addiction), pathways to health equity for Aboriginal peoples (Institute of Aboriginal Peoples' Health), and population health interventions (Institute of Population and Public Health).
In November 2010, a national workshop identified research gaps and opportunities related to Food and Health, and built on a workshop INMD hosted in January 2010 called Developing a Research Agenda to Support Sodium Reduction in Canada. A number of partners contributed financially to this workshop, including the Public Health Agency of Canada, the Advanced Food and Materials Network (A Network of Centres of Excellence), the Heart and Stroke Foundation of Canada, Grand Challenges Canada, as well as a number of institutes within CIHR – the Institute of Human Development, Child and Youth Health, the Institute of Genetics (IG) and the Institute of Neurosciences, Mental Health and Addiction (INMHA).
Environments, genes and chronic disease
INMD recognizes the influence of genes and the environment on the development of chronic disease. The Institute will promote the acquisition of knowledge on the phenotypic variation of complex and rare diseases, interactions with the human microbiome, and the health consequences of changes in the natural and built environments.
This work includes advancing knowledge in the following areas:
-
Natural and built environments relating to the pathobiology of both common and rare chronic diseases
-
Evaluation of the role of environments on chronic disease (e.g., IBD, metabolic syndrome)
-
Rare diseases, understanding that this approach ultimately benefits the health of all Canadians
This priority supports the research outlined in Roadmap related to promoting health and reducing the burden of chronic disease and links to the initiatives of other CIHR institutes, including: the Human Microbiome Initiative (the Institute of Infection and Immunity), epigenetics (INMHA), Inflammation (the Institute of Musculoskeletal Health and Arthritis), and Rare Diseases (IG).
Continuum of care
INMD aims to improve the health care experience and health of people with chronic disease by fostering research on access to appropriate care, including prevention and treatment. INMD will support research on new approaches to chronic disease prevention and management (e.g., coordinate primary and specialty health care sectors), focus on transitions across different dimensions of the care and age continuum, and advance research that includes health care reform, care gaps and priority populations.
This work includes advancing knowledge by doing the following:
-
Develop new approaches to prevent and manage chronic diseases with emphasis on diabetes, kidney and digestive diseases
-
Optimize coordination between specialists and primary care providers
-
Reduce care gaps across continuum of care and the lifespan
This priority will support INMD-related research in health services. It aligns with research priorities in Roadmap related to enhancing patient-oriented care and improving clinical results, and supporting a high quality, accessible and sustainable health care system. The research priority links to the pan-CIHR Strategy on Patient-Oriented Research (SPOR), as well as to an institute-led initiative on community-based primary health care (the Institute of Health Services and Policy Research).
Obesity and healthy body weight: seeking solutions
INMD aims to support research on solution-focused interventions related to obesity at the clinical, policy and population health level. INMD will foster research on priority populations (e.g., children, Aboriginal peoples and morbidly obese individuals) and emphasize knowledge translation to improve prevention and enhance weight-management strategies.
This work includes advancing knowledge by developing the following:
-
solutions to promote healthy body weights (e.g., school-based approaches, intervention research)
-
interventions to prevent and manage obesity, including outcomes of specialized treatment services, comparative analysis of clinical outcomes for bariatric surgical procedures and increasing understanding of underlying mechanisms of action of various bariatric care options
This priority builds on INMD's past strategic initiatives and responds to stakeholders' recommendations (see Figure 1). It supports the research priorities outlined in Roadmap related to promoting health and reducing the burden of chronic disease, enhancing patient-oriented care and improving clinical results, and supporting a high quality, accessible and sustainable health care system. The research priority links to the SPOR and Population Health Interventions initiatives.
In February 2010, the president of CIHR approved INMD's strategic plan for 2010–2014. The new INMD strategic priorities align to CIHR's strategic plan, Roadmap. INMD is positioned to contribute to Government of Canada priorities in the area of food and nutrition (e.g., reducing sodium consumption) and other areas relevant to the INMD mandate.
INMD's Institute Advisory Board has developed a plan to operationalize these strategic priorities, and INMD is now pursuing related partnership opportunities. There is a high level of support for INMD's new strategic plan; many research communities have expressed their enthusiasm for INMD's leadership in broadening beyond OHBW.
In response to the 2006 International Review commentary on engaging stakeholders, in January 2009, INMD launched a monthly, two-page INMD newsletter. The newsletter is sent to more than 5,000 people in the research community, relevant voluntary health organizations and medical professional societies. It is intended to engage the community in INMD activities and inform them about new research opportunities available at CIHR. Responses to the newsletter have been exceptionally positive.
Conclusions
Over the past 10 years, INMD has contributed to the Canadian research enterprise by advancing knowledge and building capacity in obesity and healthy body weights. Canada is among the leading countries in obesity research, and Canadian investigators excel, according to internationally accepted standards of scientific excellence, in the creation of knowledge in obesity and other areas of the INMD mandate. The challenge for the future will be to actively engage the full spectrum of INMD-relevant research communities and ensure that INMD-related research flourishes in relation to the broader slate of INMD research priorities so as to advance knowledge and improve the health of Canadians.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
INMD specific
| ANCA | anti-neutrophil cytoplasmic antibody |
| ARC | average of relative citations |
| CAG | Canadian Association of Gastroenterology |
| CDA | Canadian Diabetes Association |
| CDHF | Canadian Digestive Health Foundation |
| CON | Canadian Obesity Network |
| CSN | Canadian Society of Nephrology |
| DOL | Diabetes, Obesity, Lipid & Lipoprotein Disorders |
| DREAM | Diabetes REduction Assessment with Ramipril and Rosiglitazone Medication |
| GI | Gastrointestinal |
| GLP-2 | glucagon-like peptide-2 |
| HSFC | Heart and Stroke Foundation of Canada |
| IAB | Institute Advisory Board |
| IBD | inflammatory bowel disease |
| KFOC | Kidney Foundation of Canada |
| KRESCENT | Kidney Research Scientist Core Education and National Training Program |
| MC | Montreal Classification |
| MeSH | U.S. National Library of Medicine Medical Subject Headings |
| OHBW | Obesity and Healthy Body Weight |
| OST | Observatoire des sciences et des technologies |
| RFA | request for application |
| SI | specialization index |
| SPOR | Strategy on Patient-Oriented Research |
| STIHR | Strategic Training Initiative in Health Research |
| WoS | Web of Science |
- Date modified: