The First Decade
IHDCYH staff members and co-authors of this document:
In Montreal
- Dr. Michael S. Kramer, Scientific Director
- Dr. Anne-Cécile Desfaits, Assistant Director
- Ms. Stella DiPiano, Administrative Assistant to the Scientific Director
- Ms. Anick Lambert, Project Officer
In Ottawa
- Ms. Elisabeth Fowler, Assistant Director, Partnerships and International Relations
- Ms. Lynne Renaud, Project Officer
Table of contents
- Executive summary
- Introduction
- What have we done and why have we done it?
- What have we accomplished?
- Lessons learned
- Going forward
- Acknowledgements
- Appendix A
- Appendix B
- References
- Figure 1: Percentage of CIHR overall expenditures related to IHDCYH-relevant research, by fiscal year
- Figure 2: Relative change in number of publications, Canada versus rest of the world, 1990–2008
- Figure 3: Mean number of citations of publications, Canada versus rest of the world, 1990–2006
Institute acronyms
IA: Institute of Aging
IAPH: Institute of Aboriginal Peoples’ Health
ICR: Institute of Cancer Research
ICRH: Institute of Circulatory and Respiratory Health
IG: Institute of Genetics
IGH: Institute of Gender and Health
IHSPR: Institute of Health Services and Policy Research
IHDCYH: Institute of Human Development, Child and Youth Health
III: Institute of Infection and Immunity
IMHA: Institute of Musculoskeletal Health and Arthritis
INMHA: Institute of Neurosciences, Mental Health and Addiction
INMD: Institute of Nutrition, Metabolism and Diabetes
IPPH: Institute of Population and Public Health
Executive summary
The Canadian Institutes of Health Research’s (CIHR’s) Institute of Human Development, Child and Youth Health (IHDCYH) has just completed its first 11 years. In this document, IHDCYH’s leadership summarizes the Institute’s activities, achievements, key lessons learned, and suggestions for moving forward.
The document begins with an overview of IHDCYH’s inputs (strategic funding initiatives, capacity building, and support of its research community). The following section of the report summarizes IHDCYH’s most important outputs. These include a large increase in our community’s share, on a percentage basis, of CIHR funding in open and strategic grants, career salary awards, and training awards. We also demonstrate a larger temporal increase in Canada’s (vs other countries’) number and quality of publications in both reproductive health and child and youth health, especially in the years since the advent of CIHR.
Key outputs relating to impact on clinical decisionmaking, public policy, individual behaviours, the health care system, and the Canadian economy are also summarized. A few examples of these impacts include:
- Changes in clinical practice relating to the risks of multiple courses of steroids given to the mother before birth to prevent severe respiratory disease in premature babies, and the benefits of using caffeine after birth to prevent apnea (pauses in breathing) in premature babies;
- The widespread use of “sprinkles” (micronutrients) in the developing world to improve the nutrition of infants and young children;
- The revision of WHO recommendations regarding the duration of exclusive breastfeeding;
- The increased use of helmets in skiers and snowboarders to protect against head injury;
- A reduction in wait times and improvement of behavioural outcomes for mothers and children with mental health problems in rural Nova Scotia and Ontario;
- Major changes in clinical care for newborns in neonatal intensive care units (NICU) across Canada that have decreased the length of stay in NICU by 2 days, translating into potential savings of $40M per year;
- The creation of an improved child booster seat that is more acceptable to parents and children.
The document concludes with a brief discussion of lessons learned during IHDCYH’s first 11 years: the added value of multidisciplinary collaboration, integrated knowledge translation, and financial and educational support to our research community; and the need to protect and sustain our focus on developmental processes and trajectories and their impact on health and disease across the lifecourse.
In its first decade, IHDCYH has helped build a strong, cohesive research community poised to face the reproductive and child health challenges of the 21st century.
Introduction
Mothers and children are usually healthy and, other than for neonatal intensive care, contribute little to the escalating costs of Canada’s health care system. With low and declining rates of fetal, infant, and child mortality and morbidity, arguing that more strategic research is needed in reproductive and child health might seem a “tough sell.” But since its inception, IHDCYH has seen as its strategic focus the process of development (biological, behavioural, and social), rather than the myriad diseases that can afflict mothers, children, and youth. Developmental processes operate throughout lifecourse and thus affect the entire population, not only in Canada but across the world. Unfortunately, the pre-conceptional health of parents, the biological processes underlying normal and abnormal embryonic and fetal development, preterm birth, fetal growth, prenatal and postnatal brain development, and the developmental origins of adult chronic diseases are important areas of health research that are unlikely to receive high priority for funding in other organ-, disease-, or theme- (pillar-) based Institutes.
In 2011, CIHR and its Institute of Human Development, Child and Youth Health (IHDCYH) celebrated their first 10 years of existence. This year has also marked the end of IHDCYH’s second strategic plan, and receipt of recommendations by the Expert Review Team who evaluated IHDCYH and provided input into CIHR’s 2011 International Review Panel. In early 2012, IHDCYH will transition to a new Scientific Director and a new host institution. It is thus a good time to take stock of what we at IHDCYH have done, why we have done it, what we have accomplished, what lessons we have learned along the way, and what we need to do to build on past successes and meet future challenges.
In the next section, we discuss IHDCYH’s “inputs,” including a brief description of and rationale for our major strategic initiatives (request for applications, RFAs). We also summarize the measures we have taken to build capacity and support our research community. The succeeding section will focus on our outputs, including data on funding, publications, partnerships, ethics, and impacts on decision-making and the economy. We conclude with sections on the lessons we have learned and future challenges facing reproductive and child health research in Canada.
What have we done and why have we done it?
When IHDCYH began its activities in 2001, Canada already had a vibrant, internationally recognized community of researchers in the areas of IHDCYH’s mandate, including:
- reproductive and developmental biology
- maternal-fetal endocrinology and physiology
- perinatal epidemiology
- perinatal and pediatric randomized controlled trials (RCTs)
- developmental psychology, child psychiatry, and neuroscience
IHDCYH’s early funding initiatives built on these existing strengths, rather than on filling gaps. IHDCYH’s leadership recognized the need to use its strategic budget for more than merely extending the open operating grants competition. A major strategic focus was breaking down barriers and encouraging (or even requiring) collaboration among investigators across the four research themes (“pillars”): biomedical, clinical, health services, and population health.
IHDCYH’s first strategic plan (2001-2005) highlighted six priority areas, with a plan to launch request for applications (RFAs) to support team grants in all six priorities. All RFAs required participation from multiple research themes and provided substantial funding ($750,000 per grant per year for five years). This plan was predicated on the belief that Institute strategic budgets would increase to $20–25 million a year. That amount would provide funding adequate not only to support several large team grants in each of the six strategic priorities, but also to allow other investments, including capacity building, knowledge translation (KT), and ethics. Thus, IHDCYH did not actively seek or expect co-funding partnerships with other CIHR Institutes. This philosophy led to the launch of our first two large, multidisciplinary team grant RFAs: “Healthy Gametes” and “Healthy Pregnancies.”
After the first year or two, however, CIHR’s Institute strategic budgets began to plateau, and it became fiscally impossible to implement the strategic plan as envisioned. IHDCYH’s commitment of funds for five-year grants forced the leadership to decrease the size of team grants awarded in subsequent RFAs (from $750,000 per year to $500,000 per year maximum) and to search more actively for both internal and external funding partners. Thus, IHDCYH’s third multidisciplinary team RFA (Healthy Developmental Trajectories) included participation by four other Institutes: the Institute of Gender and Health (IGH), the Institute of Neurosciences, Mental Health and Addiction (INMHA), the Institute of Nutrition, Metabolism and Diabetes (INMD), and the Institute of Population and Public Health (IPPH). It also included an external partner, Autism Speaks. Conversely, IHDCYH began to partner on strategic initiatives led by other institutes: a large team grant in pediatric palliative care (RFA led by the Institute of Cancer Research, or ICR) and smaller grants in the area of child obesity (with INMD), health inequalities (with IGH), and tobacco control (with ICR and INMHA).
In 2006, CIHR and IHDCYH underwent its first international review, and the International Review Panel (IRP) made several recommendations concerning IHDCYH. They recommended greater investment in research on birth defects and mental health, more partnerships, and improved incorporation of KT activities in our strategic initiatives.
A second strategic plan was developed in the latter part of 2005 to cover the second five years of IHDCYH’s existence, 2006-2010. In line with the IRP recommendations, the second strategic plan included an increased emphasis on integrated knowledge translation and external partnerships. It also resulted in a new priority area (unintentional and intentional injury) and a new crosscutting theme (reproductive and child health services and policy research).
Since 2006, IHDCYH has championed CHILD (the Canadian Healthy Infant Longitudinal Development) Study, a national birth cohort study co-funded with the AllerGen Network of Centres of Excellence and a number of other CIHR Institute and Canadian federal government partners to examine the role of indoor air quality in the development of asthma and allergic disease in children. IHDCYH also launched an RFA to contribute to the World Health Organization (WHO) Global Survey of Maternal and Infant Health, the initial focus of which is to assess the maternal, fetal, and infant health consequences of the large variations in cesarean delivery rates within and between countries. Canada is the only developed country to participate in this international collaborative survey. In partnership with the Holland Bloorview Kids Rehabilitation Hospital Foundation, we have funded multidisciplinary teams to develop and evaluate approaches designed to improve the quality of life in children with disabilities, and in partnership with Health Canada, the effects of endocrine-disrupting environmental contaminants on reproductive health outcomes.
Since the 2009 release of Roadmap, CIHR’s strategic plan for 2009-2014, IHDCYH has ensured that all of our RFAs have aligned not only with our own strategic priorities, but also with those of Roadmap. The latter alignment was achieved by bundling closely-related priority research topic areas and cross-cutting themes. The four priority areas that emerged were:
- Reproductive, prenatal, and maternal health
- Neurocognitive and behavioural development and mental health of children and youth
- Chronic disease (focused on obesity, asthma, childhood disability, and the developmental origins of adult chronic disease)
- Intentional and unintentional injury
The four cross-cutting priority themes were:
- The social environment
- The physical environment
- Health services
- Aboriginal and other vulnerable populations
Chronic disease, mental health, health services, and Aboriginal/vulnerable populations align directly with three of Roadmap’s five strategic priorities. In addition, intentional injury (domestic violence, child abuse, and suicide) and unintentional injury (especially motor vehicle accidents linked to alcohol or drug use) are closely linked to mental illness. Finally, exposure to environmental contaminants is explicitly mentioned in Roadmap among threats to health.
Consistent with our strategic priority on intentional and unintentional injury, IHDCYH championed STAIR (Strategic Teams in Applied Injury Research), with IHDCYH funding or co-funding five of the seven teams that were successful in that competition. In 2011, IHDCYH launched two priority announcements to fund research on improving access to mental health services for children and youth: one in CIHR’s Partnerships for Health System Improvement program, the other in Knowledge Synthesis, and launched a large RFA to establish Applied Chairs in reproductive and child health services and policy research.
A chronological list of all RFAs initiated by IHDCYH is contained in Appendix A.
Building capacity
As an institute focused on the health and development of the young, it was only natural for IHDCYH to take an active role in training and supporting new investigators in reproductive and child health and helping them get a good start in their research careers.
The National Grants Program for new principal investigators (PIs), developed in collaboration with the SickKids Foundation (SKF), was IHDCYH’s first external (to CIHR) partnership. In total, IHDCYH and SKF have funded 102 of these grants for new PIs, thus providing a major boost to the early investigative careers of child and youth health researchers in Canada.
Shortly after IHDCYH’s scientific directorship transition in May 2003, Dr. Kramer and the Institute Advisory Board (IAB) made an important change in IHDCYH’s policy with respect to priority announcements in the open operating grants program. As of March 2003, IHDCYH has limited its $100,000 (maximum) one-year grants to start-up grants for new PIs, based on criteria similar to those in our new PI grants program with SKF. Since the inception of this program, IHDCYH has funded 54 of these start-up grants. In IHDCYH’s 2006 evaluation of the program, most new PIs reported that they obtained subsequent peer-reviewed funding from CIHR and/or other peer-reviewed funding agencies. They considered the initial start-up grant from IHDCYH to be a major factor in launching their investigative careers. In some cases, the grants prevented them from leaving research altogether.
In October 2003, Dr. Kramer, along with the other CIHR Institutes’ scientific directors, visited the U.S. National Institutes of Health and held bilateral meetings with senior scientific staff there. As a result of discussions with the National Institute of Child Health and Human Development (NICHD), collaborative, week-long Summer Institutes were developed in two strategically important areas of training for both Canada and the United States: reproductive and perinatal epidemiology, and maternalfetal pharmacology. Prior to this initiative, neither country had established training programs for graduate students or postdoctoral fellows in these areas.
These Summer Institutes have been remarkably successful. Every year since 2005, approximately 20 participants have been selected for each (275 participants since their inception) from a highly competitive group of candidates from Canada, the U.S., and other countries. The week-long Summer Institutes combine lectures with small-group discussions of research protocols, debates and other interactive formats to provide intense, stimulating, and unique training experiences.
For the last several years, the two Summer Institutes have usually been held simultaneously and have provided joint learning sessions and opportunities for informal social interaction between the faculties and trainees. The Reproductive and Perinatal Epidemiology Summer Institute has spawned a new textbook co-authored by the Canadian and American faculty, which was published in February 2011.
The Summer Institute in Global Health Research is an initiative of the Canadian Coalition for Global Health Research, in collaboration with the Institute of Population and Public Health and several other CIHR Institutes, including IHDCYH. Its objectives are to nurture the next generation of global health researchers, facilitate North-South partnerships, and promote “action research.” IHDCYH has participated in all of these Summer Institutes since 2005 and was a major organizer and funding partner in the sixth Summer Institute (held in Burkina Faso in 2009), which focused on maternal and child health research.
IHDCYH has invested heavily in the initial and renewal rounds of the Strategic Training Initiative in Health Research (STIHR) program. One IHDCYH-funded STIHR grant that deserves special mention is the Canadian Child Health Clinician Scientist Program, which is co-funded by IHDCYH and external partners. This unique program trains and supports new clinician-investigators in child and youth health research at the PhD, postdoctoral, and new investigator career stages. The program provides support and multidisciplinary networking for practicing clinicians from diverse backgrounds, including medicine, nursing, psychology, physical and occupational therapy, and dietetics. Clinician scientists from a variety of clinical disciplines provide a rich mentoring network for this highly successful training program.
Supporting our community
One of the important messages we received from focus groups and other consultations during the evolution and development of our second strategic plan was a need to build a more cohesive reproductive and child health community in Canada. We therefore developed a program of investigator-initiated research planning and dissemination workshop grants, travel awards for trainees, lectureships, and skills update awards for new and more senior investigators. IHDCYH also instituted a series of career development seminars in conjunction with regular annual scientific meetings of the Western and Eastern Perinatal Research Societies and the Canadian Fertility and Andrology Society. These seminars include sessions on grantsmanship, publication, ethics, knowledge translation, mentorship, and work-life balance.
Perhaps even more useful than these awards and grants have been IHDCYH’s interactions with our communities and academic institutions across the country during the IAB’s biannual face-to-face meetings. In conjunction with those IAB meetings, IHDCYH collaborates with local researchers to organize half-day workshops, scientific presentations, and informal social gatherings to ensure two-way communication between these local research communities and the IHDCYH leadership. Together, these activities have increased cohesion in Canada’s reproductive and child health community.
As an Institute focused on the health and development of the young, IHDCYH has succeeded in training, nurturing, and supporting the careers of many new investigators in reproductive and child health.
What have we accomplished?
Funding
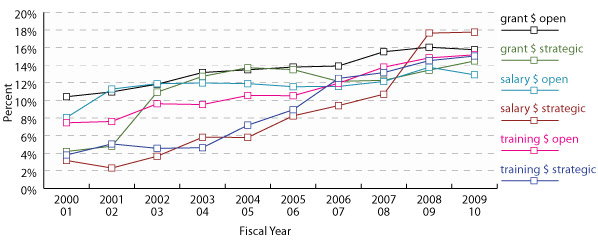
As shown in Figure 1, funding for grants, salary awards, and training awards in reproductive and child health has increased substantially since the creation of CIHR in 2000–2001. The data are expressed as percentages of overall CIHR expenditure in each category and thus demonstrate the relative growth of reproductive and child health research. These data show continued growth in open and strategic funding of grants, salary awards, and training awards. In dollars, funding from 2000–2001 to 2009–2010 increased from $25.7M to $73.8M for open grants, from $1.3M to $34.6M for strategic grants, from $2.0M to $2.3M for open salary awards, from $0.1M to $2.0M for strategic salary awards, from $2.2M to $8.1M for open training awards and from $0.1 to $2.7M for strategic training awards. Since the categories of strategic funding include strategic initiatives launched by other CIHR Institutes and by CIHR “central,” these data indicate substantial leverage of non-IHDCYH CIHR open and strategic funding by IHDCYH’s research community.
Figure 1: Percentage of CIHR overall expenditures related to IHDCYH-relevant research, by fiscal year
Publications
Given the increase in funding, it is not surprising that the number of Canadian publications related to IHDCYH’s mandate has also increased. Much research published by Canadian investigators in reproductive and child health is funded by sources other than CIHR and some is likely to be unfunded. Thus, caution is advised in inferring a direct causal relationship between CIHR (or IHDCYH) funding and Canadian publications.
With the help of Dr. KS Joseph, a former IHDCYH IAB member, separate bibliometric analyses were conducted for reproductive health and for child and youth health. Although some publications included both areas of IHDCYH’s mandate (and are thus included in both analyses), the two are separated chronologically by the occurrence of the first breath. “Reproductive health” includes reproductive biology, fertility/infertility, developmental biology, embryology/teratology, pregnancy, fetal death, and childbirth. “Child and youth health” comprises all health research on newborns, infants, children, and youth. These bibliometric analyses are based on the PubMed and Web of Science databases, using medical subject heading (MeSH) terms to identify relevant publications, and the authorship address field to ensure that at least one of each publication’s authors was affiliated with a Canadian institution.
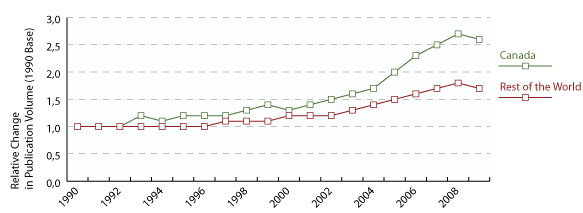
Figures 2a and 2b summarize the relative changes in number of publications (with 1990 as baseline) in these areas between 1990 and 2008 from Canada versus the rest of the world. The data show an increase across the globe, but the rise in Canada is clearly higher than in the rest of the world, with increased separation since the advent of CIHR.
Figure 2: Relative change in number of publications, Canada versus rest of the world, 1990–2008
a. Reproductive health
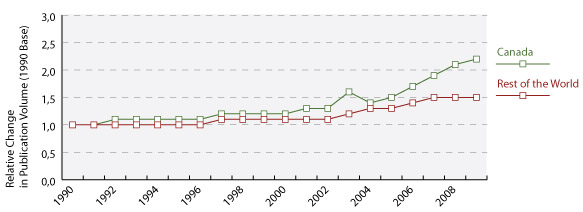
b. Child and youth health
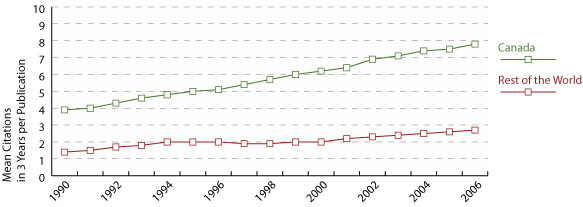
Figures 3a and 3b show the trend in mean citations, within three years of publication, per article related to reproductive health and child and youth health published by authors from Canada versus the rest of the world from 1990 to 2006 (instead of 2008, to allow 3 full years for citations through the end of 2009). Although the number of citations has increased slightly in the rest of the world, the rate of increase has been far higher in Canada, doubling from 1990 to 2006. Again, the separation between Canada and the rest of the world has increased since the advent of CIHR. These data indicate that beyond the increase in number of publications shown in Figures 3a and 3b, their quality relative to the rest of the world has also increased.
As another index of publication quality, the proportion of publications with at least one Canadian author among the 500 most highly cited papers between 1990 and 2008 increased from approximately 5% to 8% for reproductive health and from 6% to 8% for child and youth health during this 18-year period.
Canadian reproductive and child health researchers have increased their relative (to CIHR overall) grant funding, as well as the quantity and quality of their publications.
Figure 3: Mean number of citations of publications, Canada versus rest of the world, 1990–2006
a. Reproductive health
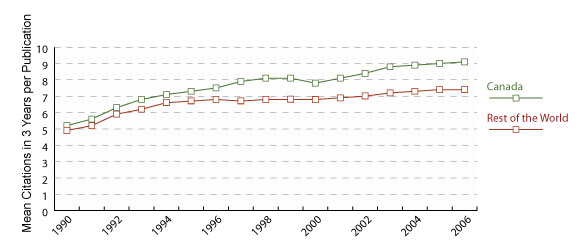
b. Child and youth health
Partnerships
Because of the plateau in the Institute’s strategic budget and our wish to increase impact on decision-making, IHDCYH has greatly increased its partnerships since the 2006 International Review report. IHDCYH has partnered with all 12 of the other CIHR Institutes, the Knowledge Translation Branch, and the Ethics Office. IHDCYH-led strategic initiatives have benefited from $20.8M in internal partnerships and have leveraged $25.0M from external partners. IHDCYH has also contributed $1.7M to initiatives led by other institutes, which have leveraged an additional $2.3M from external partners.
A list of funding and decision-making partners participating in IHDCYH’s strategic initiatives is included in Appendix A, while those initiatives on which IHDCYH was a funding partner are contained in Appendix B.
Ethics
A major challenge of child and youth research is to ensure that advances are achieved in a way that maximizes benefits, minimizes potential harm, and respects parental authority and the developing autonomy of minors. Most of the ethical norms governing research involving human subjects do not take a clear position on child and youth research. They usually indicate in a general manner that children and adolescents should be included in research without providing further guidance. The increasing demand to include children and adolescents in research areas such as genomics, randomized trials of new drug therapies, and cohort (longitudinal) studies requires new and updated ethical guidance that keeps pace with the possibilities of emerging technology.
In collaboration with CIHR’s Ethics Office, McGill University’s Centre of Genomics and Policy, the National Council on Ethics in Human Research, the Public Health Agency of Canada, Health Canada, and MICYRN, IHDCYH has funded and logistically supported the development of a document that proposes best practices for research involving children and youth. With an extensive inventory of current international thinking and protocols, this landmark document addresses the particular ethical and legal issues raised by current and emerging trends in child and youth research, and proposes practical solutions for researchers and research ethics boards.1
Impact
CIHR-funded research in reproductive and child health has not only created new knowledge (as revealed by the important publications cited below), but has also facilitated the translation of that knowledge, with important impacts on clinical decisionmaking, public policy, individual behaviours, the health care system, and the economy.
Clinical deision-making
Based on the most recent data available, the number and total value of IHDCYH-affiliated randomized controlled trials (RCTs) in the area of reproductive and child health have been second only to those affiliated with the Institute of Circulatory and Respiratory Health since the inception of CIHR. Several of these RCTs have had important impacts on clinical decision-making:
- The Caffeine for Apnea of Prematurity trial (PI: Dr. Barbara Schmidt, McMaster University) showed that not only did caffeine treatment of very preterm infants lead to a reduced risk of bronchopulmonary dysplasia (chronic lung disease of prematurity) during the newborn hospitalization,2 but also increased the likelihood of surviving without developmental disability by the end of the second year of life.3 This trial received the inaugural Trial of the Year award from the Society for Clinical Trials and has led to routine use of caffeine therapy among very preterm infants, not only in Canada but internationally.
- Dr. William Fraser of the University of Montreal led an international, multicentre RCT that demonstrated the ineffectiveness of amnioinfusion (saline infused into the amniotic cavity), which had been thought to reduce the risk of meconium aspiration syndrome by diluting the concentration of meconium in the inspired amniotic fluid.4 The results led to the widespread discontinuation of this previously common clinical practice.
- The Multiple Courses of Antenatal Corticosteroids trial, led by Dr. Kellie Murphy of the University of Toronto, showed that multiple courses of antenatal steroids did not reduce mortality or morbidity from respiratory distress syndrome in preterm infants, and resulted in restricted fetal growth, including birth weight and length and head circumference.5 These results led to a sharp reduction in the multiple courses of antenatal steroids previously used in Canada and internationally.
Public policy
CIHR-funded research has also had a major impact on public policy in the area of reproductive and child health:
- Dr. Dave Ellemberg and his team from the University of Montreal demonstrated that children and youth who sustain sports-related concussion injuries continue to have mild neurological deficits up to a year after the original injury.6, 7 This research led to major changes in return-to-play policies, thus ensuring that Canadian children and youth can safely resume contact sports.
- Dr. Stanley Zlotkin, a pediatric nutritionist from Toronto’s SickKids Hospital, has developed a small sachet called Sprinkles containing a day’s supply of powdered iron and other micronutrients, including zinc and vitamin A, that can be added to any semi-liquid food, including porridge or yogurt, without changing its taste, colour, or texture.8 Sprinkles has reached four million at-risk children in more than 30 countries, and its distribution has been promoted by the WHO, the World Food Program, and UNICEF.
- Dr. Joan Bottorff and her team from the University of British Columbia have focused on smoking and tobacco reduction in the context of women’s interactions and relationships with their partners.9 This research has informed Health Canada guidelines that support pregnant women and new mothers to reduce and stop smoking. Information from one of the booklets developed from this project has also been adapted for use by the U.S. National Cancer Institute, Tobacco Control Branch in its website for pregnant smokers.
- Dr. Michael Kramer at McGill University was asked by WHO to carry out a systematic review of evidence on the optimal duration of exclusive breastfeeding.10 Part of that systematic review was based on his and his colleagues’ cluster-randomized trial of a breastfeeding promotion intervention in the Republic of Belarus. That trial and the sub sequent systematic review led the World Health Assembly to revise its recommendation for the optimal duration of exclusive breastfeeding to six months (from four to six months).
Individual behaviours
CIHR-funded research in the area of reproductive and child health has also had a measurable impact on decision-making involving behaviours by the general public, particularly in the area of injury prevention:
- Dr. Anne Snowdon and her team at the University of Windsor developed an educational program, Bobby Shooster Rides Safely in His Booster, which included a children’s storybook, a growth chart to identify a correct safety seat for a child’s height and weight, and a DVD to help parents correctly install safety seats. They demonstrated increases in knowledge, and in the correct use of booster seats, one year after the intervention.11
- Dr. Brent Hagel and his colleagues at McGill University and the University of Calgary have published landmark research12 and systematic reviews13 demonstrating the efficacy of helmet use by skiers and snowboarders in protecting against head injury. These investigators have also shown that, despite conventional wisdom, helmets do not increase the risk of neck injury. These results have been widely publicized and likely have contributed to increased helmet use by skiers and snowboarders in Canada and abroad.
Health care system
- Dr. Patrick McGrath’s CIHR-funded team from Dalhousie University developed a new program (Strongest Families) that provides greater access to mental health services for mothers and children for problems ranging from maternal postpartum depression to child anxiety and attention deficit/hyperactivity.14 This research has markedly reduced wait times and improved behavioural outcomes for children and families living in rural and remote areas of Nova Scotia and in one health district in Ontario. The families report excellent satisfaction with the improved access to convenient and effective interventions for their children, and administrators are pleased with the cost-effectiveness of these programs.
- Dr. Gideon Koren of Toronto’s SickKids Hospital and the University of Toronto has developed a new screening procedure for fetal alcohol spectrum disorder (FASD) in Canada based on measuring fatty acid ethyl esters found in meconium obtained in the first two or three days of birth.15 This test has been adopted by the Public Health Agency of Canada as a screening tool for FASD. In partnership with the Canadian Association of Pediatric Health Centres, it is now being tested at various sites across the country.
- Dr. Shoo Lee (now at the University of Toronto) and his colleagues in the Canadian Neonatal Network carried out a cluster-randomized trial of two interventions, one to reduce the risk of neonatal sepsis, the other to reduce the risk of bronchopulmonary dysplasia (chronic lung disease of prematurity), in 12 neonatal intensive care units (NICUs) across Canada.16 The trial was based on an innovative, network-wide approach to designing and implementing the two experimental interventions. The results have led to major changes in clinical care in NICUs across the country.
Economy
- The above-mentioned trial from the Canadian Neonatal Network has decreased average NICU length of stay by two days, translating into potential savings of $40M per year. The network has also compared outcomes for retinopathy of prematurity (ROP) at the various sites participating in the Network with widely differing practices for screening.17 Their results should reduce by 50% the number of preterm infants routinely screened for ROP and thereby reduce health care costs by more than one million dollars per year in Network NICUs.
- The Neonatal Network has also patented a new clinical measurement tool called the SNAP II, an improvement over the original SNAP (score for neonatal acute physiology).18 The new tool is becoming an international standard for assessing severity of neonatal illness and comparing outcomes from hospital to hospital. SNAP II has been licensed to insurance companies and has already had an impact on insurance reimbursement based on illness severity.
- Dr. Anne Snowdon and her colleagues at the University of Windsor not only succeeded in improving parents’ use of car booster seats (see above), but also worked with Magna International to design and manufacture the Clek, an improved booster seat that is more acceptable to children than conventional seats and thus more likely to be used. The Clek, launched in Canada in 2006 and in the U.S. in 2007, has won several national and international awards.
CIHR and IHDCYH have responded to their knowledge translation (KT) mandate by funding and/or facilitating research that has impacted on decision-making by clinicians, policy-makers, and the general public, on the health care system, and on the Canadian economy.
Lessons learned
We are confident that some of the lessons IHDCYH has learned in its first 10 years will continue to guide the future leadership. One of IHDCYH’s earliest and most successful efforts was its emphasis on multidisciplinary, multi-theme research collaboration. Such collaboration was rare under the Medical Research Council, as individual researchers had little motivation, or even opportunity, to collaborate with scientists from other disciplines and themes. While it is too early to tell whether such collaboration has a greater impact on health and health care, this strategic effort has already been lauded by researchers from across disciplines and themes as intellectually stimulating, creative, and innovative and has led to new knowledge and new applications of that knowledge.
A second important lesson is that true knowledge translation benefits from, and may even require, integrated KT, rather than end-of-grant KT. It is difficult and often futile to attempt to apply new knowledge when that knowledge was created without the participation of decision-makers (be they the general public, health care providers, or policy-makers) in posing the research questions, choosing the research methods, and analyzing and interpreting the resulting data. IHDCYH and its Institute partners agree that involving such decisionmakers at the very earliest stages of RFA development is essential to increase the likelihood that research findings actually influence decisions. When decisionmakers co-fund these initiatives, their financial stake increases the likelihood that the research will succeed and that findings will be applied. Increasingly, such decision-makers work outside the health sector (e.g., education, social services, and justice). This is particularly important for an institute such as IHDCYH, which has few opportunities for commercial partnerships. Pharmaceutical companies, for example, tend to avoid developing and testing new drugs for pregnant women and children for fear of unforeseen adverse effects and costly litigation.
A third important lesson has been the importance of supporting IHDCYH’s research community. It will be important for IHDCYH’s future leadership to build a strong and cohesive reproductive and child health research community in Canada. Through our collaborative grants program with the SickKids Foundation, priority announcements in CIHR’s Open Operating Grants Program, Summer Institutes, and careerdevelopment workshops, IHDCYH is recognized across the country for its efforts to support trainees and new PIs in reproductive and child health. IHDCYH has also strengthened its national profile by its presence at, and contribution to, Canadian scientific and clinical meetings in the areas of the Institute’s mandate through such activities such as judging poster competitions, awarding prizes, and offering KT and scientific seminars on specific topics. Continuing these forms of support will help us achieve our mission to improve the health and health care of mothers, children, and youth in Canada and beyond.
Going forward
The Expert Review Team that evaluated IHDCYH during CIHR’s 2011 international review recommended a continued effort to obtain funding for a national pregnancy/birth cohort study, with a focus on both the physical and the social environments and their effects on long-term child health and development.19 In 2007, IHDCYH made a concerted effort to obtain additional funding for such a long-term study, outside of the CIHR base budget. Although unsuccessful, it is probably useful to consider other strategies, including the strategy utilized by the Institute of Aging for the Canadian Longitudinal Study of Aging. Perhaps IHDCYH should announce a request for proposals and help the successful applicants to seek infrastructure support from other agencies (such as the Canadian Foundation for Innovation). The unique aspects of the Canadian physical environment (particularly agricultural exposures, those related to cold temperatures, and exposure to oil sands and other petroleum industry-related contaminants and pollutants) should enable Canadian investigators to design a study that will not only answer unique and important questions for the health of Canadian mothers and children, but also be useful to other countries facing similar environmental challenges.
The Expert Review Team strongly endorsed IHDCYH’s new emphasis on reproductive and child health services and policy research. It is hoped that IHDCYH’s contribution to Community-Based Primary Health Care (one of the “Signature Initiatives” that CIHR has developed to implement the strategic priorities announced in Roadmap), and its recently-launched RFAs on improving access to mental health services for children and youth and on creating Applied Chairs in reproductive and child health services and policy research, will go a long way to filling the current gaps in this research area. The latter program in particular will not only fund the salary of mid-career investigators, but will also require universities to replace the salary that is gained for the Chair by hiring trainees and/or new investigators to work with the Chair and thereby create a “critical mass” of excellence in this strategically important area.
One of the important features of the strategic funding landscape for a number of years to come will be CIHR’s Signature Initiatives. IHDCYH has already indicated its financial commitment to three of them: Epigenetics, Community-Based Primary Health Care, and Pathways to Equity for Aboriginal Peoples.
But it remains important for IHDCYH to maintain its focus on human development, including biological, neurocognitive, behavioural, and social development. Many of CIHR’s Signature Initiatives could be stretched to include aspects related to reproductive and child health, but pediatricians and other child health professionals have often had to remind their colleagues that children are not merely “small adults.” IHDCYH’s important strategic priorities related to human reproduction, healthy pregnancy, and the developmental origins of chronic disease and of mental illness do not fit well with some of the existing Signature Initiatives. If Canada’s future generations are to profit from IHDCYH’s accomplishments, IHDCYH should build on past strengths and continue its focus on human development while taking advantage of new scientific discoveries and emerging issues in the Canadian social and health care environment.
IHDCYH has helped build a strong, cohesive research community poised to face the reproductive and child health challenges of the 21st century, not only in Canada but internationally.
Acknowledgements
IHDCYH would not be where it is today without the dedicated work of the many people who have contributed to its development over the course of the past 10 years. The inaugural Institute team at the University of Toronto, previous Ottawa-based staff, past McGill-based staff, and past and current members of our diverse and dynamic IAB are listed below.
Past IHDCYH Staff
Inaugural IHDCYH Team (University of Toronto)
- Dr. John R.G. Challis (Scientific Director)
- Nicola McDermott (Assistant Director)
- Jocelyne Arès (Executive Assistant)
- Denise Moretto (Event Coordinator)
Ottawa-Based Staff
Assistant Directors
- Diane Allen
- Louise Poulin
- Pierre Turcotte
- Loretta Wong
Project Officers
- Amanda Devost
- Gwendoline Malo
Montreal-Based Staff
- Lindsay Wallace (Administrative Assistant)
Current IHDCYH advisory board members
Chair:
- Dr. Jean-Marie Moutquin, Université de Sherbrooke (member since 2008, Chair since 2009)
Members:
- Mrs. Leanne Boyd, Healthy Child Manitoba Office (since 2011)
- Dr. Astrid Guttmann, University of Toronto (since 2010)
- Dr. Ellen Hodnett, University of Toronto (since 2008)
- Dr. Bonnie Leadbeater, University of Victoria (since 2010)
- Mrs. Karen Lloyd, Health Canada (since 2009)
- Dr. Stephen J. Lye, University of Toronto (since 2008)
- Dr. Peter Mitchell, University of Alberta (since 2008)
- Dr. Gina Muckle, Université Laval (since 2009)
- Mrs. Elaine Orrbine, Canadian Association of Paediatric Health Centres (since 2010)
- Dr. Bernard Robaire, McGill University (since 2010)
- Dr. Reg Sauve, University of Calgary (since 2009)
- Dr. Anne Snowdon, University of Windsor (since 2010)
- Dr. Charlotte Waddell, Simon Fraser University (since 2010)
Past IHDCYH advisory board members
Chairs:
- Dr. Michael S. Kramer, McGill University (2001-03)
- Mrs. Lynne Krepart, Canadian Foundation for Women’s Health, (member 2001-04, Chair 2003-04)
- Dr. Bruce Murphy, Université de Montréal (member 2003-06, Chair 2004-06)
- Dr. Victor Han, University of Western Ontario (member 2004-10, Chair 2006-09)
Members:
- Dr. Jane Drummond, University of Alberta (2001-03)
- Dr. Peter Gluckman, University of Aukland, New Zealand (2001-03)
- Dr. Jean Lafrance, University of Calgary (2001-03)
- Dr. Dan Offord, McMaster University (2001-03)
- Dr. Aubrey James Tingle, University of British Columbia (2001-03)
- Dr. Richard Tremblay, Université de Montréal (2001-03)
- Dr. Sylvain Chemtob, Université de Montréal (2003-04)
- Dr. Harvey Guyda, McGill University (2003-04)
- Dr. Bryan Richardson, University of Western Ontario (2003-04)
- Dr. Kathleen Cranley Glass, McGill University (2003-05)
- Dr. Patrick McGrath, Dalhousie University (2003-05)
- Dr. Jim Bonta, Public Safety (2003-06)
- Dr. Catherine McCourt, Health Canada (2003-06)
- Dr. Bonnie Stevens, University of Toronto (2003-06)
- Mrs. Dawn Walker, Health Canada (2003-06)
- Dr Hugh O’Brodovich, University of Toronto (2003-07)
- Dr. Peter Rosenbaum, McMaster University (2003-07)
- Dr. James M. Roberts, University of Pittsburgh, Pennsylvania (2003-07)
- Dr. Sandra Davidge, University of Alberta (2003-08)
- Dr. Shoo Lee, University of Alberta (2003-08)
- Mrs. Brenda Kirtzinger, Prairie North Health Region (2004-07)
- Dr. William Fraser, Université de Montréal (2004-08)
- Dr. Lucie Jeannotte, Université Laval (2004-09)
- Dr. Maureen Heaman, University of Manitoba (2005-08)
- Dr. K.S. Joseph, Dalhousie University (2005-09)
- Dr. Paul Glover, Health Canada (2006-08)
- Dr. Laura Arbour, University of Victoria (2006-10)
- Dr. Jay Baltz, University of Ottawa (2006-10)
- Dr. Claire Fortier, SickKids Foundation (2006-10)
- Dr. Peter Szatmari, McMaster University (2006-10)
- Dr. Robert Armstrong, University of British Columbia (2007-10)
- Dr. Ken Kao, Memorial University (2007-11)
- Dr. Donald Mattison, National Institute of Child Health and Human Development (2007-11)
- Dr. Rob Santos, Healthy Child Manitoba Office (2007-11)
- Mrs. Sue Milburn-Hopwood, Health Canada (2008-09)
Appendix A
IHDCYH’s strategic initiatives and priority announcements, including partners (by funding start date)
2002-03
Healthy Gametes and Great Embryos (5 years)
2003-04
Healthy Pregnancy, first launch (5 years)
Partner:
- INMHA
2004-05
Healthy Developmental Trajectories (5 years)
Partners:
- National Alliance for Autism Research
- IGH
- INMHA
- INMD
- IPPH
2005-06
Healthy Pregnancy, second launch (5 years)
Ethical, Legal and Social Issues in Studies Involving Pregnant Women and Children (3 years)
Partner:
- Ethics Office
2007-08
Quality of indoor Air and Development of Asthma and Allergies in Early Childhood (6 years)
Partners:
- AllerGen NCE
- Environment Canada
- Health Canada
- The Canada Mortgage and Housing Corporation
- ICRH
- IGH
- IG
- III
Maternal, Fetal and Infant consequences of Variation in Rates of Caesarean Delivery (3 years)
Partners:
- Public Health Agency of Canada
- World Health Organization
2008-09
Child and Youth Health Indicators (3 years)
Partners:
- Holland Bloorview Kids Rehabilitation Hospital Foundation
- Child Health BC and BC Child and Youth Health Research Network
- Canadian Child and Youth Health Coalition
- Provincial Centre of Excellence for Child and Youth Mental Health at CHEO
- Public Health Agency of Canada - Health Surveillance & Epidemiology Division
- IGH
- IHSPR
- INMHA
Bright Futures for Kids with Disabilities (3 years)
Partners:
- Holland Bloorview Kids Rehabilitation Hospital Foundation
- Ontario Neurotrauma Foundation
- IAPH
- IMHA
2009-10
Environmental Contaminants and Reproductive Health (5 years)
Partner:
- Health Canada
Mental Health and Addiction in Children and Youth (4 years)
Partners:
- Academy of Finland
- INMHA
Secondary Analysis of Provincial and National Databases in Maternal and Child Health, first launch (2 years)
Partners:
- IAPH
- First Nations and Inuit Health Branch
- Public Health Agency of Canada - Health Surveillance and Epidemiology Division
Strategic Teams in Applied Injury Research (5 years)
Partners:
- Alberta Centre for Child, Family and Community Research
- Alberta Innovates – Health Solutions
- Auto 21 Centre of Excellence
- Child Welfare League of Canada
- Natural Sciences and Engineering Research Council of Canada
- Ontario Neurotrauma Foundation
- Public Health Agency of Canada - Strategic Initiatives and Innovations Directorate
- Public Health Agency of Canada - Promotion and Chronic Disease Prevention Branch
- SMARTRISK
- Transport Canada
- University of Windsor
- Women and Children Health Research Institute (Alberta)
- CIHR Corporate
- CIHR Knowledge Translation Branch
- CIHR Commercialization Branch
- IA
- IGH
- IHSPR
- IMHA
2010-11
China-Canada Collaborative Teams in Health Research (3 years)
Partners:
- Ministry of Science and Technology of the People’s Republic of China
- IA
- ICR
- IG
- III
- IMHA
- INMD
- INMHA
Early Origins of Addiction in Children and Youth (4 years)
Partners:
- Academy of Finland
- INMHA
India-Canada Joint Research Program on Obesity (5 years)
Partners:
- Indian Council of Medical Research
- INMD
2011-12
Maternal Health: From Pre-Conception to the Empty Nest (5 years)
Partners:
- Alberta Centre for Child, Family and
- Community Research
- Canadian Women’s Health Network
- Health Canada – Gender and Health Unit
- Public Health Agency of Canada – Health Surveillance & Epidemiology Division
- IAPH
- IGH
Secondary Analysis of Population-Based Databases, second launch (2 years)
Partners:
- First Nations Information Governance Centre
- Public Health Agency of Canada
- Statistics Canada
- Drug Safety and Effectiveness Network
- IA
- IAPH
- IHSPR
- INMHA
- IPPH
2012-13 (initiatives launched in 2011-12)
Applied Chairs in Reproductive, Child and Youth Health Services and Policy Research (5 years)
Partners:
- Canadian Association of Paediatric Health Centres
- Fonds de recherche du Québec-Santé
- Hearth & Stroke Foundation of Canada
- IAPH
Knowledge Synthesis Grants: Access to Mental Health Services for Children and Youth (priority announcement, 1 year)
Partners:
- Mental Health Commission of Canada
- INMHA
Partnerships for Health System Improvement: Access to Mental Health Services for Children and Youth (priority announcement, 3 years)
Partners:
- Fonds de recherche du Québec-Santé
- Mental Health Commission of Canada
- Saskatchewan Health Research Foundation
Ongoing programs
New Investigator Research Grants with SickKids Foundation (3 years, since 2002-03)
Partner:
- SickKids Foundation
Start-up Grants for New Investigators (priority announcement, 1 year, since 2003-04)
Salary Awards for New Investigator in Reproductive & Child Health (priority announcement, 5 years, since 2007-08)
Appendix B
Strategic initiatives of other institutes and external funders (IHDCYH as partner)
2001-02
- New Emerging Teams, first launch (Lead: CIHR Corporate, 5 years)
- Strategic Training Initiative in Health Research, first launch (Lead: CIHR Corporate, 6 years)
2002-03
- Gene Therapy for Neurological Diseases (Lead: INMHA, 4 years)
- Global Health Research (Lead: IPPH, 1 year)
- New Emerging Teams, second launch (Lead: CIHR Corporate, 5 years)
- Reducing Health Disparities (Lead: IGH, 1 year)
2003-04
- Canadian Tobacco Control Research Initiative (Leads: ICR and INMHA, 1 year)
- Environmental Approaches to Physical Activity (Lead: INMD, 1 year)
- Global Health Research (Lead: IPPH, 1 year)
- Obesity and Healthy Body Weights (Lead: INMD, 1 year)
- Reducing Health Disparities (Lead: IGH, 1 year)
- Strategic Training Initiative in Health Research, second launch (Lead: CIHR Corporate, 6 years)
2004-05
- Aboriginal Health, New Researchers (Lead: IAPH, 5 years)
- Canadian Language and Literacy Research Network (1 year)
- Canadian Tobacco Control Research Initiative (Leads: ICR and INMHA, 1 year)
- Childhood Obesity (Lead: INMD, 3 years)
- Facing our Future: Human Genetics, Ethics, Law and Society (Lead: IG, 1 year)
- New Perspectives on Gender and Health (Lead: IGH, 1 year)
- Palliative and End-of-Life Care (Lead: ICR, 5 years)
- Rural Health (Lead: IAPH, 1 year)
- Target Obesity: Doctoral Research Awards
- (Lead: INMD, 3 years)
2005-06
- Canadian Cochrane Centre (5 years)
- Collaborative Health Research Program (Lead: Natural Sciences and Engineering Research Council of Canada, 3 years)
- Fellowships in Health Disparities (Leads: IGH and IPPH, 2 years)
- Fellowships in Global Health (Lead: IPPH and III, 2 years)
- Genomic Medicine and Human Development (Lead: IG, 5 years)
- Health Disparities (Lead: IGH, 3 years)
- Japan-Canada Joint Health Research Initiative (Lead: INMHA, 2 years)
- Population and Public Health Research Methods and Tools (Lead: IPPH, 1 year)
- Research in Addictions (Lead: INMHA, 1 year)
- Toward Enhanced Quality of Life Through Injury Prevention (Lead: IHSPR, 1 year)
2006-07
- Complementary and Alternative Health Care (Lead: SickKids Foundation, 2 years)
- Doctoral Research Award in Genetics (Ethics, Law, and Society) (Lead: IG, 3 years)
- Doctoral Research Award in Public Health (Lead: IPPH, 3 years)
- Early Life Events (Lead: INMHA, 5 years)
- Health Disparities (Lead: IGH, 5 years)
- Japan-Canada Joint Health Research Initiative (Lead: INMHA, 2 years)
- Mexico-Canada Joint Health Research Program in Tuberculosis (Lead: ICRH, 2 years)
- National Anti-Drug Strategy (Lead: INMHA, 5 years)
- Research Exchange and Impact for System Support (Lead: Canadian Health Services Research Foundation, 3 years)
2007-08
- Chairs in Public Health (Lead: IPPH, 5 years)
- Built Environment, Obesity, and Health (Lead: Heart & Stroke Foundation of Canada, 3 years)
- Canadian Tobacco Control Research Initiative (Leads: ICR and INMHA, 5 years)
- Fellowships in Health Services and Policy Research (Lead: IHSPR, 4 years)
- Japan-Canada Joint Health Research Initiative (Lead: INMHA, 2 years)
2008-09
- Brain Disorders in the Developing World (Lead: INMHA, 2 years)
- Childhood Obesity Prevention (Lead: INMD, 3 years)
- Doctoral Research Awards and Fellowships in Public Health (Lead: IPPH, 2 years)
- First Nations Regional Longitudinal Health Survey Secondary Data Analysis (Lead: IAPH, 2 years)
- Intervention Research in Childhood Obesity (Lead: INMD, 2 years)
- Knowledge Translation in Mental Health and Addiction (Lead: INMHA, 5 years)
- Partnerships for Health System Improvement (Lead: IHSPR, 3 years)
2009-10
- Cancer Survivorship (Lead: ICR, 1 year)
- Evidence on Tap: Expedited Knowledge Synthesis (Lead: IHSPR and CIHR Knowledge Translation Branch, 1 year)
- Health Systems Research on H1N1 (Lead: IPPH, 1 year)
- Partnerships for Health System Improvement (Lead: IHSPR, 3 years)
- Post-Market Drug Safety and Effectiveness (Lead: Drug Safety and Effectiveness Network, 1 year)
- Primary and Community-Based Healthcare (Lead: IHSPR, 1 year)
- Sleep and Circadian Rhythms (Lead: ICRH, 5 years)
- Strategic Training Initiative in Health Research, third launch (Lead: CIHR Corporate, 6 years)
2010-11
- Climate Change and Adaptation (Lead: International Development Research Centre, 5 years)
2011-12 (as of November 2011)
- Official Language Minority Communities (Lead: CIHR Official Language Minority Communities Initiative, 1 year)
- Programmatic Grants to Tackle Health and Health Equity (Lead: IPPH, 5 years)
Ongoing programs
- Built Environment, Obesity, and Health (since 2009-10) (Lead: Heart & Stroke Foundation of Canada, 3 years)
- China-Canada Joint Health Research Initiative (since 2006-07) (Lead: INMHA, 3 years)
- Knowledge Synthesis Grants (since 2008-09) (Lead: CIHR Knowledge Translation Branch, 1 year)
References
- Canadian Institutes of Health Research. Best Practices for Research Involving Children and Adolescents [Internet]. 2010. Available from Canadian Institutes of Health Research
- Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, et al. Caffeine therapy for apnea of prematurity. N Engl J Med 2006;354(20):2112-2121.
- Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, et al. Long-term effects of caffeine therapy for apnea of prematurity. N Engl J Med 2007;357(19):1893-1902.
- Fraser WD, Hofmeyr J, Lede R, Faron G, Alexander S, Goffinet F, et al. Amnioinfusion for the prevention of the meconium aspiration syndrome. N Engl J Med 2005;353(9):909-917.
- Murphy KE, Hannah ME, Willan AR, Hewson SA, Ohlsson A, Kelly EN, et al. Multiple courses of antenatal corticosteroids for preterm birth (MACS): a randomized controlled trial. Lancet 2008;372(December 20/27):2143-2151.
- Boutin D, Lassonde M, Robert M, Vanassing P, Ellemberg D. Neurophysiological assessment prior to and following sports-related concussion during childhood: a case study. Neurocase 2008;14:239-248.
- Ellemberg D, Leclerc S, Couture S, Daigle C. Prolonged neuropsychological impairments following a first concussion in female university soccer athletes. Clin J Sport Med 2007;17(5):369-374.
- Zlotkin SH, Schauer C, Christofides A, Sharieff W, Tondeur MC, Hyder SM. Micronutrient sprinkles to control childhood anaemia. PloS Med 2005;2(1):e1.
- Bottorff JL, Oliffe J, Kalaw C, Carey J, Mroz L. Men’s constructions of smoking in the context of women’s tobacco reduction during pregnancy and postpartum. Soc Sci Med 2006;62(12):3096-3108.
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews 2002, Issue 1. Art. No.: CD003517. DOI:10.1002/14651858.CD003517.
- Snowdon AW, Hussein A, Purc-Stevenson R, Follo G, Ahmed E. A longitudinal study of the effectiveness of a multimedia intervention on parents’ knowledge and use of vehicle safety systems for children. Accident Analysis and Prevention 2009;41:498-505.
- Hagel BE, Pless IB, Goulet C, Platt RW, Robitaille Y. Effectiveness of helmets in skiers and snowboarders: casecontrol and case crossover study. BMJ 2005;330(7486):345-349.
- Russell K, Christie J, Hagel BE. The effect of helmets on the risk of head and neck injuries among skiers and snowboarders: a meta-analysis. CMAJ 2010;182(4):333-340.
- McGrath PJ, Lingley-Pottie P, Thurston C, MacLean C, Cunningham C, Waschbusch DA, Watters C, Stewart S, Bagnell A, Santor D, Chaplin W. Telephone-based mental health interventions for child disruptive behavior or anxiety disorders: randomized trials and overall analysis. Am Acad Child Adolesc Psychiatry 2011; 50(11):1162-72.
- Gareri J, Lynn H, Handley M, Rao C, Koren G. Prevalence of fetal ethanol exposure in a regional population-based sample by meconium analysis of fatty acid ethyl esters. Ther Drug Monit 2008;30:239-245.
- Lee SK, Aziz K, Singhal N, Cronin CM, James A, Lee DSC, et al. Improving the quality of care for infants: a cluster randomized controlled trial. CMAJ 2009;181(8):469-476.
- Lee SK, Normand C, McMillan D, Ohlsson A, Vincer M, Lyons C; Canadian Neonatal Network. Evidence for changing guidelines for routine screening for retinopathy of prematurity. Arch Pediatr Adolesc Med 2001;155(3):387-395.
- Skarsgard ED, MacNab YC, Qiu Z, Little R, Lee SK; Canadian Neonatal Network. SNAP-II predicts mortality among infants with congenital diaphragmatic hernia. J Perinatol 2005;25(5):315-319.
- Canadian Institutes of Health Research. Inventory of Pregnancy and Birth Cohort Studies [Internet]. 2010. Available from: Canadian Institutes of Health Research
- Date modified: